
Page 8 - Food Bank Council 2020 Renewal Booklet
P. 8
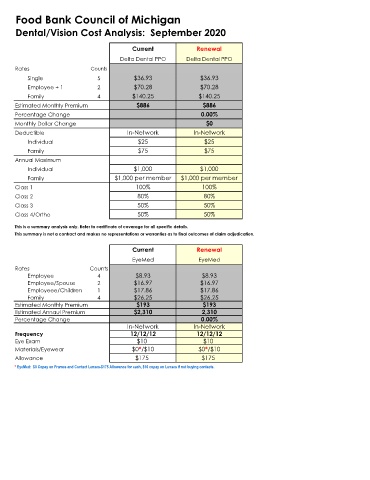
Food Bank Council of Michigan
Dental/Vision Cost Analysis: September 2020
Current Renewal
Delta Dental PPO Delta Dental PPO
Rates Counts
Single 5 $36.93 $36.93
Employee + 1 2 $70.28 $70.28
Family 4 $140.25 $140.25
Estimated Monthly Premium $886 $886
Percentage Change 0.00%
Monthly Dollar Change $0
Deductible In-Network In-Network
Individual $25 $25
Family $75 $75
Annual Maximum
Individual $1,000 $1,000
Family $1,000 per member $1,000 per member
Class 1 100% 100%
Class 2 80% 80%
Class 3 50% 50%
Class 4/Ortho 50% 50%
This is a summary analysis only. Refer to certificate of coverage for all specific details.
This summary is not a contract and makes no representations or warranties as to final outcomes of claim adjudication.
Current Renewal
EyeMed EyeMed
Rates Counts
Employee 4 $8.93 $8.93
Employee/Spouse 2 $16.97 $16.97
Employeee/Children 1 $17.86 $17.86
Family 4 $26.25 $26.25
Estimated Monthly Premium $193 $193
Estimated Annaul Premium $2,310 2,310
Percentage Change 0.00%
In-Network In-Network
Frequency 12/12/12 12/12/12
Eye Exam $10 $10
Materials/Eyewear $0*/$10 $0*/$10
Allowance $175 $175
* EyeMed: $0 Copay on Frames and Contact Lenses-$175 Allowance for each, $10 copay on Lenses if not buying contacts.