
Page 3 - Tetra Renewal 2020
P. 3
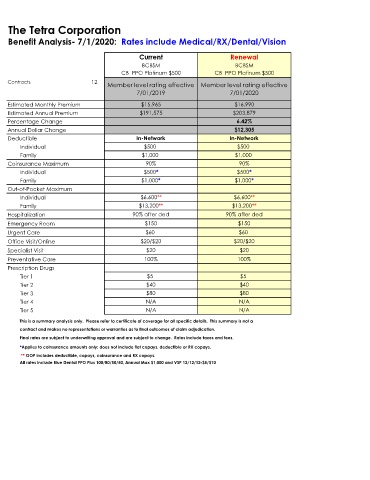
The Tetra Corporation
Benefit Analysis- 7/1/2020: Rates include Medical/RX/Dental/Vision
Current Renewal
BCBSM BCBSM
CB PPO Platinum $500 CB PPO Platinum $500
Contracts 12
Member level rating effective Member level rating effective
7/01/2019 7/01/2020
Estimated Monthly Premium $15,965 $16,990
Estimated Annual Premium $191,575 $203,879
Percentage Change 6.42%
Annual Dollar Change $12,305
Deductible In-Network In-Network
Individual $500 $500
Family $1,000 $1,000
Coinsurance Maximum 90% 90%
Individual $500* $500*
Family $1,000* $1,000*
Out-of-Pocket Maximum
Individual $6,600** $6,600**
Family $13,200** $13,200**
Hospitalization 90% after ded 90% after ded
Emergency Room $150 $150
Urgent Care $60 $60
Office Visit/Online $20/$20 $20/$20
Specialist Visit $20 $20
Preventative Care 100% 100%
Prescription Drugs
Tier 1 $5 $5
Tier 2 $40 $40
Tier 3 $80 $80
Tier 4 N/A N/A
Tier 5 N/A N/A
This is a summary analysis only. Please refer to certificate of coverage for all specific details. This summary is not a
contract and makes no representations or warranties as to final outcomes of claim adjudication.
Final rates are subject to underwriting approval and are subject to change. Rates include taxes and fees.
*Applies to coinsurance amounts only; does not include flat copays, deductible or RX copays.
** OOP includes deductible, copays, coinsurance and RX copays.
All rates include Blue Dental PPO Plus 100/80/50/50, Annual Max $1,000 and VSP 12/12/12-$5/$10