
Page 5 - LBC 2020 Renewal Proposal
P. 5
LANSING BREWING COMPANY
OCTOBER 1, 2020 MEDICAL RENEWAL
PREPARED BY: GREGORY D. BROGAN
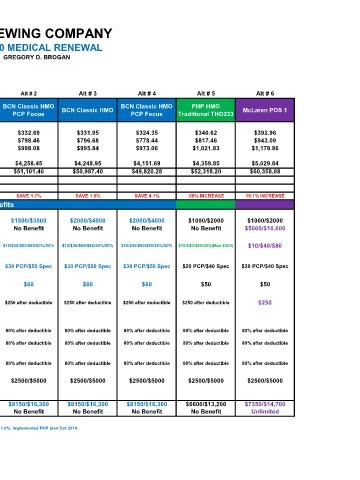
Current Renewal Alt # 1 Alt # 2 Alt # 3 Alt # 4 Alt # 5 Alt # 6
# of BCN Classic HMO BCN Classic HMO BCN Classic HMO BCN Classic HMO BCN Classic HMO BCN Classic HMO PHP HMO McLaren POS 1
employees PCP Focus PCP Focus Traditional THO233
Single 5 $338.38 $361.59 $340.48 $332.69 $331.95 $324.35 $340.62 $392.96
Two Person 2 $812.11 $867.80 $817.15 $798.46 $796.68 $778.44 $817.46 $943.09
Family 1 $1,015.14 $1,084.75 $1,021.43 $998.08 $995.84 $973.06 $1,021.83 $1,178.86
Estimated Monthly Premium 8 $4,331.26 $4,628.30 $4,358.13 $4,258.45 $4,248.95 $4,151.69 $4,359.85 $5,029.84
Estimated Annual Premium $51,975.12 $55,539.60 $52,297.56 $51,101.40 $50,987.40 $49,820.28 $52,318.20 $60,358.08
Total Est. Annual Premium
Change in Premium 6.86% INCREASE .62% INCREASE SAVE 1.7% SAVE 1.9% SAVE 4.1% .66% INCREASE 16.1% INCREASE
Benefits
Deductible
In network $1000/$2000 $1000/$2000 $1500/$3000 $1500/$3000 $2000/$4000 $2000/$4000 $1000/$2000 $1000/$2000
Out Network No Benefit No Benefit No Benefit No Benefit No Benefit No Benefit No Benefit $5000/$10,000
Prescription drug copay $4/$15/$40/$80/20%/20% $4/$15/$40/$80/20%/20% $10/$30/$60/$80/20%/20% $10/$30/$60/$80/20%/20% $10/$30/$60/$80/20%/20% $10/$30/$60/$80/20%/20% $15/$40/$80/20%(Max.$300) $10/$40/$80
Office visit copay $20 PCP/$40 Spec $20 PCP/$40 Spec $30 PCP/$50 Spec $30 PCP/$50 Spec $30 PCP/$50 Spec $30 PCP/$50 Spec $20 PCP/$40 Spec $20 PCP/$40 Spec
Urgent care copay $50 $50 $60 $60 $60 $60 $50 $50
Emergency Room Copay $250 after deductible $250 after deductible $250 after deductible $250 after deductible $250 after deductible $250 after deductible $250 after deductible $250
Hospitalization
In patient 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible
Out patient 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible
Lab & X-ray 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible
Embedded Coinsurance Max. $2500/$5000 $2500/$5000 $2500/$5000 $2500/$5000 $2500/$5000 $2500/$5000 $2500/$5000 $2500/$5000
Maximum copayment
In network $6600/$13,200 $6600/$13,200 $8150/$16,300 $8150/$16,300 $8150/$16,300 $8150/$16,300 $6600/$13,200 $7350/$14,700
Out network No Benefit No Benefit No Benefit No Benefit No Benefit No Benefit No Benefit Unlimited
2019 rates increased .37%
2018 moved to large group and rates increased 1.2%, 2017 group moved to BCN and saved 11.4%, 2016 increased ded/copays and rates increased 1.6%, Implemented PHP plan Oct 2015
Prepared June 2020