
Page 103 - QCS.19 SPD - HSA
P. 103
What You Will Pay
Common Limitations, Exceptions, & Other
Services You May Need Network Provider Out-of-Network Provider
Medical Event Important Information
(You will pay the least) (You will pay the most)
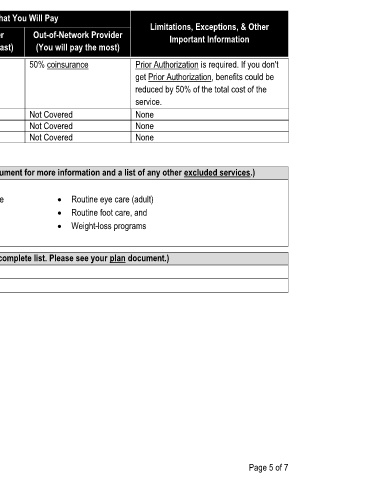
Hospice service 0% coinsurance 50% coinsurance Prior Authorization is required. If you don't
get Prior Authorization, benefits could be
reduced by 50% of the total cost of the
service.
Children's eye exam Not Covered Not Covered None
If your child needs
Children's glasses Not Covered Not Covered None
dental or eye care
Children's dental check-up Not Covered Not Covered None
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
· Acupuncture · Long-term care
· Bariatric surgery · Non-emergency care when traveling outside the · Routine eye care (adult)
· Cosmetic surgery United States · Routine foot care, and
· Dental care (adult) · Private-duty nursing · Weight-loss programs
· Infertility treatment
Other Covered Services (Limitations may apply to these services. This isn't a complete list. Please see your plan document.)
· Chiropractic care
· Hearing aids
Page 5 of 7