
Page 3 - PWH.19 Employee Benefits
P. 3
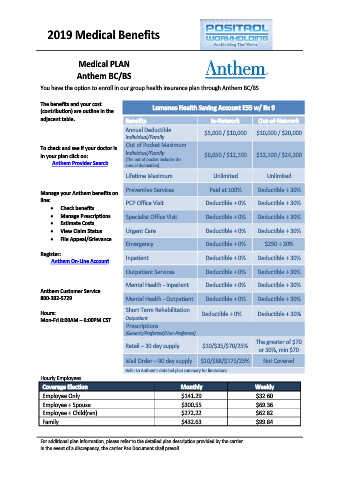
2019 Medical Benefits
Medical PLAN
Anthem BC/BS
You have the option to enroll in our group health insurance plan through Anthem BC/BS.
The benefits and your cost Lumenos Health Saving Account E55 w/ Rx 9
(contribution) are outline in the
adjacent table. Benefits InNetwork OutofNetwork
Annual Deductible $5,000 / $10,000 $10,000 / $20,000
Individual/Family
Out of Pocket Maximum
To check and see if your doctor is
in your plan click on: Individual/Family $6,050 / $12,100 $12,100 / $24,200
(The out of pocket includes the
Anthem Provider Search annual deductible)
Lifetime Maximum Unlimited Unlimited
Preventive Services Paid at 100% Deductible + 30%
Manage your Anthem benefits on
line: PCP Office Visit Deductible + 0% Deductible + 30%
x Check benefits
x Manage Prescriptions Specialist Office Visit Deductible + 0% Deductible + 30%
x Estimate Costs
x View Claim Status Urgent Care Deductible + 0% Deductible + 30%
x File Appeal/Grievance
Emergency Deductible + 0% $250 + 20%
Register:
Anthem OnLine Account Inpatient Deductible + 0% Deductible + 30%
Outpatient Services Deductible + 0% Deductible + 30%
Mental Health Inpatient Deductible + 0% Deductible + 30%
Anthem Customer Service
8003825729 Mental Health Outpatient Deductible + 0% Deductible + 30%
Short Term Rehabilitation
Hours: Deductible + 0% Deductible + 30%
MonFri 8:00AM – 6:00PM CST Outpatient
Prescriptions
(Generic/Preferred/Non-Preferred)
The greater of $70
Retail – 30 day supply $10/$35/$70/25%
or 50%, min $70
Mail Order – 90 day supply $10/$88/$175/25% Not Covered
Refer to Anthem’s detailed plan summary for limitations
Hourly Employees
Coverage Election Monthly Weekly
Employee Only $141.29 $32.60
Employee + Spouse $300.55 $69.36
Employee + Child(ren) $272.22 $62.82
Family $432.63 $99.84
For additional plan information, please refer to the detailed plan description provided by the carrier.
In the event of a discrepancy, the carrier Pan Document shall prevail.