
Page 97 - QCS.19 SPD - PPO
P. 97
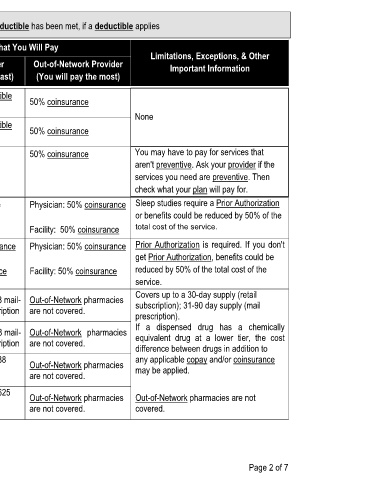
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies
What You Will Pay
Common Limitations, Exceptions, & Other
Services You May Need Network Provider Out-of-Network Provider
Medical Event Important Information
(You will pay the least) (You will pay the most)
Primary care visit to treat an $30 copay/visit deductible
injury or illness does not apply 50% coinsurance
None
Specialist visit $60 copay/visit deductible
If you visit a health 50% coinsurance
does not apply
care provider's office
or clinic Preventive care/screening/ No Charge 50% coinsurance You may have to pay for services that
immunization aren't preventive. Ask your provider if the
services you need are preventive. Then
check what your plan will pay for.
Diagnostic test (x-ray, blood Physician: No Charge Physician: 50% coinsurance Sleep studies require a Prior Authorization
If you have a test
work) or benefits could be reduced by 50% of the
Facility: No Charge Facility: 50% coinsurance total cost of the service.
Imaging (CT/PET scans, MRIs) Physician: 0% coinsurance Physician: 50% coinsurance Prior Authorization is required. If you don't
get Prior Authorization, benefits could be
Facility: 0% coinsurance Facility: 50% coinsurance reduced by 50% of the total cost of the
service.
Covers up to a 30-day supply (retail
$15 retail copay or $38 mail- Out-of-Network pharmacies
Tier 1 drugs subscription); 31-90 day supply (mail
order copay per prescription are not covered.
If you need drugs to prescription).
treat your illness or $35 retail copay or $88 mail- Out-of-Network pharmacies If a dispensed drug has a chemically
condition Tier 2 drugs equivalent drug at a lower tier, the cost
order copay per prescription are not covered.
difference between drugs in addition to
More information about $75 retail copay or $188 Out-of-Network pharmacies any applicable copay and/or coinsurance
prescription drug Tier 3 drugs mail-order copay per may be applied.
are not covered.
coverage is available at prescription
www.myallsavers.com $250 retail copay or $625 Out-of-Network pharmacies Out-of-Network pharmacies are not
Tier 4 drugs mail-order copay per are not covered. covered.
prescription
Page 2 of 7