
Page 19 - RTF.20 Employee Benefits
P. 19
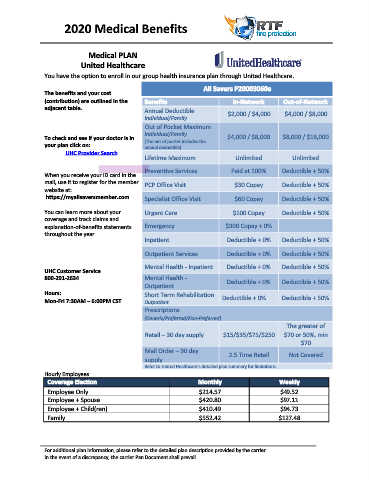
2020 Medical Benefits
Medical PLAN
United Healthcare
You have the option to enroll in our group health insurance plan through United Healthcare.
All Savers P20003060e
The benefits and your cost
(contribution) are outlined in the Benefits In‐Network Out‐of‐Network
adjacent table. Annual Deductible
Individual/Family $2,000 / $4,000 $4,000 / $8,000
Out of Pocket Maximum
To check and see if your doctor is in Individual/Family $4,000 / $8,000 $8,000 / $16,000
(The out of pocket includes the
your plan click on: annual deductible)
UHC Provider Search
Lifetime Maximum Unlimited Unlimited
Preventive Services Paid at 100% Deductible + 50%
When you receive your ID card in the
mail, use it to register for the member PCP Office Visit $30 Copay Deductible + 50%
website at:
https://myallsaversmember.com. Specialist Office Visit $60 Copay Deductible + 50%
You can learn more about your Urgent Care $100 Copay Deductible + 50%
coverage and track claims and
explanation‐of‐benefits statements Emergency $300 Copay + 0%
throughout the year.
Inpatient Deductible + 0% Deductible + 50%
Outpatient Services Deductible + 0% Deductible + 50%
Mental Health ‐ Inpatient Deductible + 0% Deductible + 50%
UHC Customer Service
800‐291‐2634 Mental Health ‐
Outpatient Deductible + 0% Deductible + 50%
Hours: Short Term Rehabilitation
Mon‐Fri 7:30AM – 6:00PM CST Outpatient Deductible + 0% Deductible + 50%
Prescriptions
(Generic/Preferred/Non‐Preferred)
The greater of
Retail – 30 day supply $15/$35/$75/$250 $70 or 50%, min
$70
Mail Order – 90 day
2.5 Time Retail Not Covered
supply
Refer to United Healthcare’s detailed plan summary for limitations
Hourly Employees
Coverage Election Monthly Weekly
Employee Only $214.57 $49.52
Employee + Spouse $420.80 $97.11
Employee + Child(ren) $410.49 $94.73
Family $552.42 $127.48
For additional plan information, please refer to the detailed plan description provided by the carrier.
In the event of a discrepancy, the carrier Pan Document shall prevail.