
Page 20 - RTF.20 Employee Benefits
P. 20
2020 Vision Benefits
United Healthcare Vision Plan
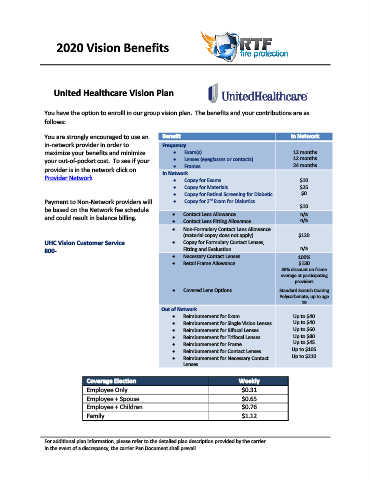
You have the option to enrolll in our group vision plan. The benefits and your contributions are as
follows:
You are strongly encouraged to use an Benefit In Network
in‐network provider in order to Frequency
maximize your benefits and minimize Exam(s) 12 months
your out‐of‐pocket cost. To see if your Lenses (eyeglasses or contacts) 12 months
provider is in the network click on Frames 24 months
In Network
Provider Network Copay for Exams $10
Copay for Materials $25
Copay for Retinal Screening for Diabetic $0
nd
Payment to Non‐Network providers will Copay for 2 Exam for Diabetics
$10
be based on the Network fee schedule n/a
and could result in balance billing. Contact Lens Allowance n/a
Contact Lens Fitting Allowance
Non‐Formulary Contact Lens Allowance
(material copay does not apply) $120
UHC Vision Customer Service Copay for Formulary Contact Lenses,
800‐ Fitting and Evaluation n/a
Necessary Contact Lenses 100%
Retail Frame Allowance $130
30% discount on frame
overage at participating
providers
Covered Lens Options Standard Scratch Coating
Polycarbonate, up to age
19
Out of Network
Reimbursement for Exam Up to $40
Reimbursement for Single Vision Lenses Up to $40
Reimbursement for Bifocal Lenses Up to $60
Reimbursement for Trifocal Lenses Up to $80
Reimbursement for Frame Up to $45
Reimbursement for Contact Lenses Up to $105
Reimbursement for Necessary Contact Up to $210
Lenses
Coverage Election Weekly
Employee Only $0.31
Employee + Spouse $0.65
Employee + Children $0.76
Family $1.12
For additional plan information, please refer to the detailed plan description provided by the carrier.
In the event of a discrepancy, the carrier Pan Document shall prevail.