
Page 69 - REMOVABLE ORTHODONTIC APPLIANCES
P. 69
Class I malocclusions 61
the canine without contacting the gingivae or
tooth. It should then pass over the canine-
premolar contact point again to follow the
gingival margin of the canine without contact-
ing it. Finally the wire should finish lingually in
the mid-line.
Cold-cured acrylic (2-3 mm in thickness) is
laid down over the wire buccally and lingually.
It extends no further than the distal surfaces of
the laterals. Dentine coloured acrylic is aesthet-
ically most acceptable.
Clinical treatment
The appliance is inserted and adjusted to
ensure suitable activation. Because the teeth
have been moved during the making of the
working model the appliance will probably not
require activation at this stage. The patient is
instructed to wear the appliance full time
except for meals and sport. At subsequent
appointments activation can be carried out by
adjusting the distal wire loops so as to approx-
imate further the lingual and labial acrylic
bars.
Where local adjustments are necessary,
appropriate trimming and the addition of small
areas of cold-cured acrylic will be effective.
When tooth movement is complete the passive
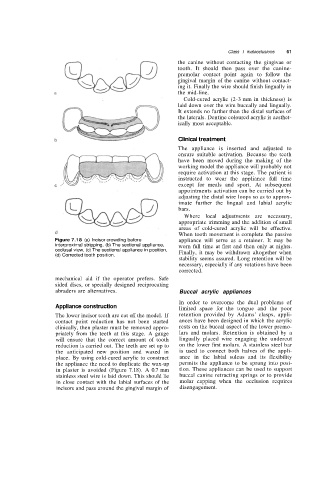
Figure 7.18 (a) Incisor crowding before appliance will serve as a retainer. It may be
interproximal stripping, (b) The sectional appliance, worn full time at first and then only at nights.
occlusal view, (c) The sectional appliance in position, Finally, it may be withdrawn altogether when
(d) Corrected tooth position.
stability seems assured. Long retention will be
necessary, especially if any rotations have been
corrected.
mechanical aid if the operator prefers. Safe
sided discs, or specially designed reciprocating
abraders are alternatives. Buccal acrylic appliances
In order to overcome the dual problems of
Appliance construction
limited space for the tongue and the poor
The lower incisor teeth are cut off the model. If retention provided by Adams' clasps, appli-
contact point reduction has not been started ances have been designed in which the acrylic
clinically, then plaster must be removed appro- rests on the buccal aspect of the lower premo-
priately from the teeth at this stage. A gauge lars and molars. Retention is obtained by a
will ensure that the correct amount of tooth lingually placed wire engaging the undercut
reduction is carried out. The teeth are set up to on the lower first molars. A stainless steel bar
the anticipated new position and waxed in is used to connect both halves of the appli-
place. By using cold-cured acrylic to construct ance in the labial sulcus and its flexibility
the appliance the need to duplicate the wax-up permits the appliance to be sprung into posi-
in plaster is avoided (Figure 7.18). A 0.7 mm tion. These appliances can be used to support
stainless steel wire is laid down. This should lie buccal canine retracting springs or to provide
in close contact with the labial surfaces of the molar capping when the occlusion requires
incisors and pass around the gingival margin of disengagement.