
Page 104 - Manual of Equine Field Surgery
P. 104
100 LIMB SURGERIES
overlapping of and tension on the instruments
bring the DDFT to, but not out of, the incision.
The DDFT is then transected with a No. 10 blade
(Figure 16-7). If the distal check ligament is
present at the level of the incision, it is isolated
and transected with the DDFT. After transection,
the heel elevation can be removed to check for
adequate gap formation between the tendon ends.
Closure of the subcutaneous tissue is optional.
Closure of the skin is performed with an inter-
rupted apposing or everting pattern using No.
2-0 monofilament suture material.
POSTOPERATIVE CARE
PqstoP,erative Care
Bandaging: A sterile dressing is placed over the
Site of
:-1---
approach incision and a half limb bandage is applied. The
limb should remain bandaged for 30 days, and
the bandage is changed every 5 to 7 days or more
frequently if needed.
i
Exetcise Restridons: Horses with laminitis
should be rested as their condition indicates and
are not allowed significant turnout for a minimum
of 6 months. Foals with contracture can be allowed
turnout in a small area after 1 week, and the
amount of exercise allowed is gradually increased
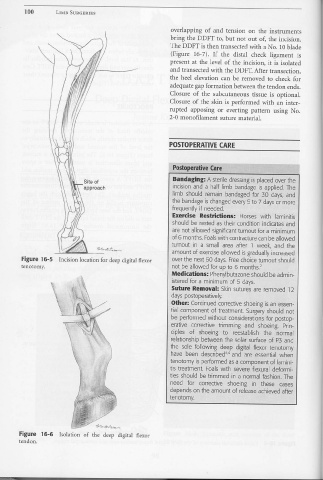
Figure 16-5 Incision location for deep digital flexor over the next 60. days. Free choice turnout should
tenotomy. not be allowed for up to 6 months. 2
Medications: Phenylbutazone should be admin-
istered for a minimum of 5 days.
J '
Suture Reme>val: Skin sutures are removed 12
days postoperatively.
Other: Continued corrective shoeing is an essen-
tial component of treatment. Surgery should not
be performed without considerations for postop-
erative corrective trimming and shoeing. Prin-
ciples of shoeing to reestablish the normal
relationship between the solar surface of P3 and
the sole following deep digital flexor tenotorny
have been describedv' and are essential when
tenotomy is performed as a component of larnini-
tis treatment. Foals with severe flexural deformi-
ties should be trimmed in a normal fashion. The
need for corrective shoeing in these cases
depends on the amount of release achieved after
tenotomy.
Figure 16-6 Isolation of the deep digital flexor
tendon.