
Page 94 - Manual of Equine Field Surgery
P. 94
90 LIMB SURGERIES
•
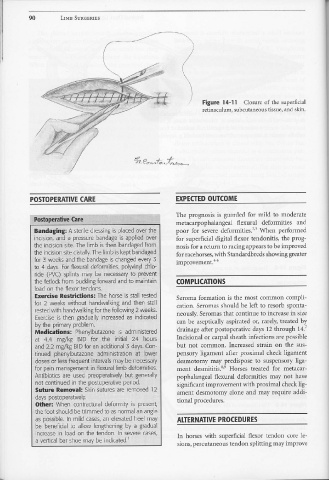
Figure 14-11 Closure of the superficial
retinaculum, subcutaneous tissue, and skin.
POSTOPERATIVE CARE EXPECTED OUTCOME
The prognosis is guarded for mild to moderate
metacarpophalangeal flexural deformities and
Bandaging: A sterile dressing is placed over .the poor for severe deformities.2•3 When performed
incision, and a pressure bandage is applied over for superficial digital flexor tendonitis, the prog-
the incision site. The limb is then bandaged from nosis for a return to racing appears to be improved
the incision site distally. The limb is kept bandaged for racehorses, with Standardbreds showing greater
for 3 weeks and the bandage is changed every 3 improvement. 4-6
to 4 days. For flexural deformities, polyvinyl chlo-
ride (PVC) splints may be n~tessary to prevent
the fetlock from buckling forward and to maintain COMPLICATIONS
load on the flexor tendons.
Exercise Restridions: The horse is stall rested Seroma formation is the most common compli-
for 2 weeks without handwalking and then stall cation. Seromas should be left to resorb sponta-
rested with handwalking for the following 2 weeks. neously. Seromas that continue to increase in size
Exercise is then gradually increased as indicated
by the primary problem. can be aseptically aspirated or, rarely, treated by
Medications: Phenylbutazone rs administered drainage after postoperative days 12 through 14.7
at 4.4 mg/kg BID for .. the initial 24 hours Incisional or carpal sheath infections are possible
and 2.2 mg/kg Bl D for an additional 3 · days . Con- but not common. Increased strain on the sus-
.
tinued phenylbutazone administration at lower pensory ligament after proximal check ligament
doses or less frequent intervals may be necessary desmotomy may predispose to suspensory liga-
for pain management in flexural limb deformities. ment desmititis.8•9 Horses treated for metacar-
Antibiotics are used preoperatively but generally pophalangeal flexural deformities may not have
not continued in the postoperative period. significant improvement with proximal check lig-
Suture Removal: Skin sutures are removed 12 ament desmotomy alone and may require addi-
days postoperatively. tional procedures.
Other: When contractural deformity is present,
the foot should be trimmed to as normal an angle
as possible. In mild cases, an elevated heel may ALTERNATIVE PROCEDURES
be beneficial to allow lengthening by a gradual
increase in load on the tendon. In severe cases, In horses with superficial flexor tendon core le-
a vertical bar shoe may be indicated.'
sions, percutaneous tendon splitting may improve