
Page 99 - Manual of Equine Field Surgery
P. 99
Distal Splint Bone Resection 95
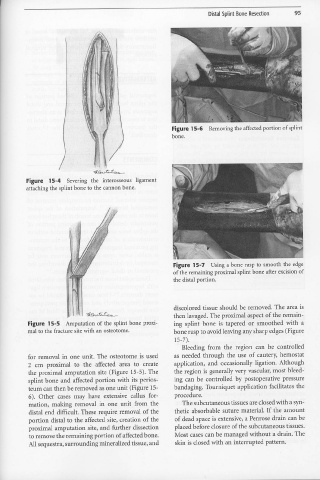
Figure 15-6 Removing the affected portion of splint
bone.
-i:;;_g&><,(.> t; J:;·Gt?t,.--.
Figure 15-4 Severing the interosseous ligament
attaching the splint bone to the cannon bone.
Figure 15- 7 Using a bone rasp to smooth the edge
of the remaining proximal splint bone after excision of
the distal portion.
. 1
I f. discolored tissue should be removed. The area is
~-~t;,.t;~. then lavaged. The proximal aspect of the remain-
Figure 15-5 Amputation of the splint bone proxi- ing splint bone is tapered or smoothed with a
mal to the fracture site with an osteotome. bone rasp to avoid leaving any sharp edges (Figure
15-7).
Bleeding from the region can be controlled
for removal in one unit. The osteotome is used as needed through the use of cautery, hemostat
2 cm proximal to the affected area to create application, and occasionally ligation. Although
the proximal amputation site (Figure 15-5). The the region is generally very vascular, most bleed-
splint bone and affected portion with its perios- ing can be controlled by postoperative pressure
teum can then be removed as one unit (Figure 15- bandaging. Tourniquet application facilitates the
6). Other cases may have extensive callus for- procedure.
mation, making removal in one unit from the The subcutaneous tissues are closed with a syn-
distal end difficult. These require removal of the thetic absorbable suture material. If the amount
portion distal to the affected site, creation of the of dead space is extensive, a Penrose drain can be
proximal amputation site, and further dissection placed before closure of the subcutaneous tissues.
to remove the remaining portion of affected bone. Most cases can be managed without a drain. The
All sequestra, surrounding mineralized tissue, and skin is closed with an interrupted pattern.