
Page 52 - Weinberg & Schwartz Allstate Brochure Flipbook
P. 52
0
Value Plan 3
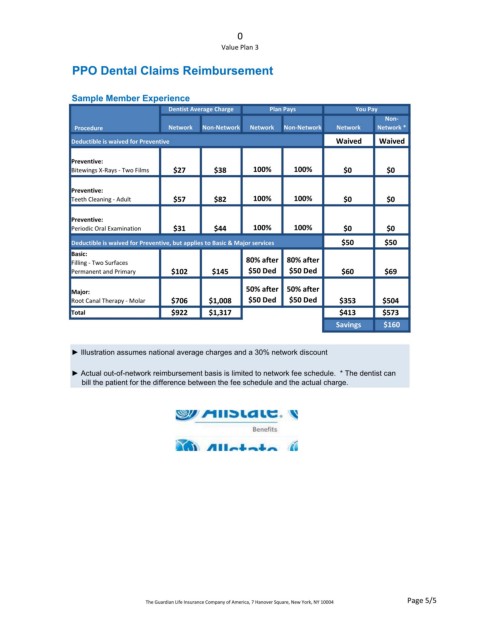
PPO Dental Claims Reimbursement
Sample Member Experience
Dentist Average Charge Plan Pays You Pay
Non
Procedure Network NonNetwork Network NonNetwork Network Network *
Deductible is waived for Preventive Waived Waived
Preventive:
Bitewings X‐Rays ‐ Two Films $27 $38 100% 100% $0 $0
Preventive:
Teeth Cleaning ‐ Adult $57 $82 100% 100% $0 $0
Preventive:
Periodic Oral Examination $31 $44 100% 100% $0 $0
Deductible is waived for Preventive, but applies to Basic & Major services $50 $50
Basic:
Filling ‐ Two Surfaces 80% after 80% after
Permanent and Primary $102 $145 $50 Ded $50 Ded $60 $69
50% after 50% after
Major:
Root Canal Therapy ‐ Molar $706 $1,008 $50 Ded $50 Ded $353 $504
Total $922 $1,317 $413 $573
Savings $160
► Illustration assumes national average charges and a 30% network discount
► Actual out-of-network reimbursement basis is limited to network fee schedule. * The dentist can
bill the patient for the difference between the fee schedule and the actual charge.
Page 5/5
The Guardian Life Insurance Company of America, 7 Hanover Square, New York, NY 10004