
Page 16 - 2021 Medical Plan SPD
P. 16
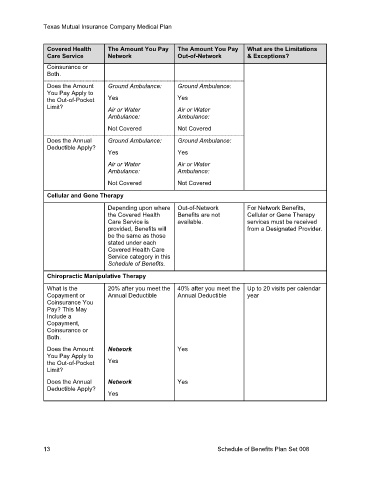
Texas Mutual Insurance Company Medical Plan
Covered Health The Amount You Pay The Amount You Pay What are the Limitations
Care Service Network Out-of-Network & Exceptions?
Coinsurance or
Both.
Does the Amount Ground Ambulance: Ground Ambulance:
You Pay Apply to
the Out-of-Pocket Yes Yes
Limit? Air or Water Air or Water
Ambulance: Ambulance:
Not Covered Not Covered
Does the Annual Ground Ambulance: Ground Ambulance:
Deductible Apply?
Yes Yes
Air or Water Air or Water
Ambulance: Ambulance:
Not Covered Not Covered
Cellular and Gene Therapy
Depending upon where Out-of-Network For Network Benefits,
the Covered Health Benefits are not Cellular or Gene Therapy
Care Service is available. services must be received
provided, Benefits will from a Designated Provider.
be the same as those
stated under each
Covered Health Care
Service category in this
Schedule of Benefits.
Chiropractic Manipulative Therapy
What Is the 20% after you meet the 40% after you meet the Up to 20 visits per calendar
Copayment or Annual Deductible Annual Deductible year
Coinsurance You
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount Network Yes
You Pay Apply to
the Out-of-Pocket Yes
Limit?
Does the Annual Network Yes
Deductible Apply?
Yes
13 Schedule of Benefits Plan Set 008