
Page 172 - Cover Letter and Evaluation for Sue Marx
P. 172
2/7/2019 Your Medicare Health Plan Details
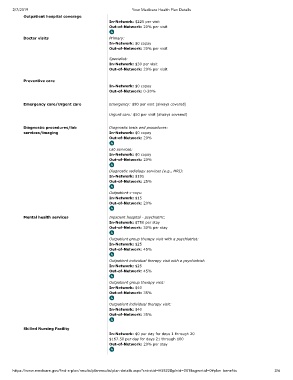
Outpatient hospital coverage
In-Network: $225 per visit
Out-of-Network: 20% per visit
Doctor visits Primary:
In-Network: $0 copay
Out-of-Network: 30% per visit
Specialist:
In-Network: $30 per visit
Out-of-Network: 20% per visit
Preventive care
In-Network: $0 copay
Out-of-Network: 0-20%
Emergency care/Urgent care Emergency: $90 per visit (always covered)
Urgent care: $50 per visit (always covered)
Diagnostic procedures/lab Diagnostic tests and procedures:
services/imaging In-Network: $0 copay
Out-of-Network: 20%
Lab services:
In-Network: $0 copay
Out-of-Network: 20%
Diagnostic radiology services (e.g., MRI):
In-Network: $195
Out-of-Network: 25%
Outpatient x-rays:
In-Network: $15
Out-of-Network: 20%
Mental health services Inpatient hospital - psychiatric:
In-Network: $750 per stay
Out-of-Network: 30% per stay
Outpatient group therapy visit with a psychiatrist:
In-Network: $25
Out-of-Network: 45%
Outpatient individual therapy visit with a psychiatrist:
In-Network: $25
Out-of-Network: 45%
Outpatient group therapy visit:
In-Network: $40
Out-of-Network: 35%
Outpatient individual therapy visit:
In-Network: $40
Out-of-Network: 35%
Skilled Nursing Facility
In-Network: $0 per day for days 1 through 20
$167.50 per day for days 21 through 100
Out-of-Network: 20% per stay
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H5522&plnid=001&sgmntid=0#plan_benefits 2/6