
Page 175 - Cover Letter and Evaluation for Sue Marx
P. 175
2/7/2019 Your Medicare Health Plan Details
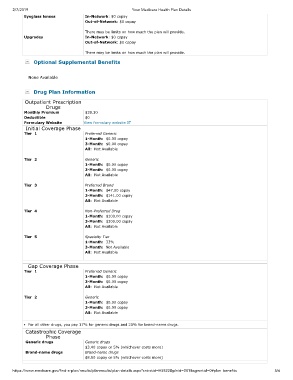
Eyeglass lenses In-Network: $0 copay
Out-of-Network: $0 copay
There may be limits on how much the plan will provide.
Upgrades In-Network: $0 copay
Out-of-Network: $0 copay
There may be limits on how much the plan will provide.
Optional Supplemental Benefits
None Available
Drug Plan Information
Outpatient Prescription
Drugs
Monthly Premium $39.30
Deductible $0
Formulary Website View formulary website
Initial Coverage Phase
Tier 1 Preferred Generic
1-Month: $0.00 copay
3-Month: $0.00 copay
All: Not Available
Tier 2 Generic
1-Month: $0.00 copay
3-Month: $0.00 copay
All: Not Available
Tier 3 Preferred Brand
1-Month: $47.00 copay
3-Month: $141.00 copay
All: Not Available
Tier 4 Non-Preferred Drug
1-Month: $100.00 copay
3-Month: $300.00 copay
All: Not Available
Tier 5 Specialty Tier
1-Month: 33%
3-Month: Not Available
All: Not Available
Gap Coverage Phase
Tier 1 Preferred Generic
1-Month: $0.00 copay
3-Month: $0.00 copay
All: Not Available
Tier 2 Generic
1-Month: $0.00 copay
3-Month: $0.00 copay
All: Not Available
For all other drugs, you pay 37% for generic drugs and 25% for brand-name drugs.
Catastrophic Coverage
Phase
Generic drugs Generic drugs
$3.40 copay or 5% (whichever costs more)
Brand-name drugs Brand-name drugs
$8.50 copay or 5% (whichever costs more)
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H5522&plnid=001&sgmntid=0#plan_benefits 5/6