
Page 13 - Cover Letter and Medicare Evaluation for Diane Falten
P. 13
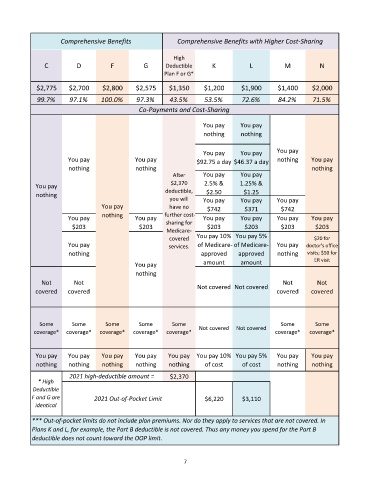
Comprehensive Benefits Comprehensive Benefits with Higher Cost-Sharing
High
C D F G Deductible K L M N
Plan F or G*
$2,775 $2,700 $2,800 $2,575 $1,350 $1,200 $1,900 $1,400 $2,000
99.7% 97.1% 100.0% 97.3% 43.5% 53.5% 72.6% 84.2% 71.5%
Co-Payments and Cost-Sharing
You pay You pay
nothing nothing
You pay You pay You pay
You pay You pay $92.75 a day $46.37 a day nothing You pay
nothing nothing nothing
After You pay You pay
You pay $2,370 2.5% & 1.25% &
nothing deductible, $2.50 $1.25
you will You pay You pay You pay
You pay have no $742 $371 $742
You pay nothing You pay further cost- You pay You pay You pay You pay
sharing for
$203 $203 $203 $203 $203 $203
Medicare-
covered You pay 10% You pay 5% $20 for
You pay services. of Medicare- of Medicare- You pay doctor's office
nothing approved approved nothing visits; $50 for
You pay amount amount ER visit
nothing
Not Not Not covered Not covered Not Not
covered covered covered covered
Some Some Some Some Some Some Some
coverage* coverage* coverage* coverage* coverage* Not covered Not covered coverage* coverage*
You pay You pay You pay You pay You pay You pay 10% You pay 5% You pay You pay
nothing nothing nothing nothing nothing of cost of cost nothing nothing
2021 high-deductible amount = $2,370
* High
Deductible
F and G are 2021 Out-of-Pocket Limit $6,220 $3,110
identical
*** Out-of-pocket limits do not include plan premiums. Nor do they apply to services that are not covered. In
Plans K and L, for example, the Part B deductible is not covered. Thus any money you spend for the Part B
deductible does not count toward the OOP limit.
7