
Page 11 - Cover Letter and Medicare Evaluation for Neill McLauchlin
P. 11
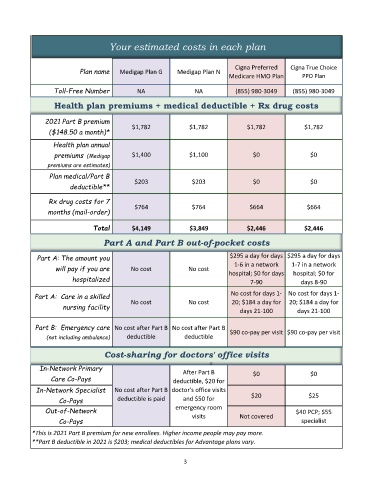
Your estimated costs in each plan
Cigna Preferred Cigna True Choice
Plan name Medigap Plan G Medigap Plan N
Medicare HMO Plan PPO Plan
Toll-Free Number NA NA (855) 980-3049 (855) 980-3049
Health plan premiums + medical deductible + Rx drug costs
lity ratings from
Medicare web site
2021 Part B premium
($148.50 a month)* $1,782 $1,782 $1,782 $1,782
Health plan annual
premiums (Medigap $1,400 $1,100 $0 $0
premiums are estimates)
Plan medical/Part B
deductible** $203 $203 $0 $0
Rx drug costs for 7
months (mail-order) $764 $764 $664 $664
Total $4,149 $3,849 $2,446 $2,446
Part A and Part B out-of-pocket costs
Part A: The amount you $295 a day for days $295 a day for days
1-6 in a network
will pay if you are No cost No cost hospital; $0 for days 1-7 in a network
hospital; $0 for
hospitalized 7-90 days 8-90
Part A: Care in a skilled No cost for days 1- No cost for days 1-
nursing facility No cost No cost 20; $184 a day for 20; $184 a day for
days 21-100 days 21-100
Part B: Emergency care No cost after Part B No cost after Part B $90 co-pay per visit $90 co-pay per visit
(not including ambulance) deductible deductible
Cost-sharing for doctors' office visits
=
In-Network Primary After Part B $0 $0
Care Co-Pays deductible, $20 for
In-Network Specialist No cost after Part B doctor's office visits $20 $25
Co-Pays deductible is paid and $50 for
Out-of-Network emergency room $40 PCP; $55
visits
Co-Pays Not covered specialist
*This is 2021 Part B premium for new enrollees. Higher income people may pay more.
**Part B deductible in 2021 is $203; medical deductibles for Advantage plans vary.
3