Page 6 - 2015 Saint Louis University Benefits Guide
P. 6
Saint Louis University
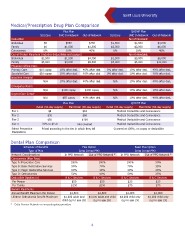
Medical/Prescription Drug Plan Comparison
Plus Plan QHDHP Plan
SLUCare UHC In-Network Out-of-Network SLUCare UHC In-Network Out-of-Network
Deductible Non-Embedded:
Individual $0 $500 $750 $1,500 $1,500 $3,000
Family $0 $1,000 $1,500 $3,000 $3,000 $6,000
Coinsurance 0% 10% 40% 0% 10% 40%
Out-of-Pocket Maximum (includes deductibles and copays) Non-Embedded:
Individual $1,500 $1,500 $4,750 $1,500 $3,000 $6,000
Family $3,000 $3,000 $9,500 $3,000 $6,000 $12,000
Physician Ofice Visits
Primary Care $10 copay 10% after ded. 40% after ded. 0% after ded. 10% after ded. 40% after ded.
Specialist Care $20 copay 10% after ded. 40% after ded. 0% after ded. 10% after ded. 40% after ded.
Inpatient Hospital
N/A 10% after ded. 40% after ded. N/A 10% after ded. 40% after ded.
Emergency Room
N/A $100 copay $100 copay N/A 10% after ded. 10% after ded.
Urgent Care Center
N/A $50 copay 40% after ded. N/A 10% after ded. 40% after ded.
Plus Plan QHDHP Plan
Retail (34-day supply) Mail Order (90-day supply) Retail (34-day supply) Mail Order (90-day supply)
Tier 1 $8 $16 Medical Deductible and Coinsurance
Tier 2 $30 $60 Medical Deductible and Coinsurance
Tier 3 $50 $100 Medical Deductible and Coinsurance
Tier 4 20% to $150 Not covered Medical Deductible and Coinsurance
Select Preventive Priced according to the tier in which they fall Covered at 100%, no copay or deductible
Medications
Dental Plan Comparison
Schedule of Beneits Flex Option Basic Plus Option
Type of Plan Delta Dental PPO Delta Dental PPO
Network Considerations In PPO Network Out of PPO Network * In PPO Network Out of PPO Network *
Coinsurance (Plan Pays)
Type A: Preventive Care 100% 100% 100% 50%
Type B: Basic Restorative Services 90% 70% 70% 35%
Type C: Major Restorative Services 60% 40% 40% 20%
Type D: Orthodontics 50% 40% 50% 25%
Deductible (Applies to) B & C Services B & C Services B & C Services B & C Services
Per Person $50 $50 $25 $25
Per Family $150 $150 $75 $75
Beneit Maximums
Annual Beneit Maximum Per Person $1,500 $1,500 $1,000 $1,000
Lifetime Orthodontia Beneit Maximum $1,000 adult and $1,000 adult and child $1,000 child only $1,000 child only
child (up to age 26) (up to age 26) (up to age 19) (up to age 19)
* Delta Premier Network or non-participating providers
6
Medical/Prescription Drug Plan Comparison
Plus Plan QHDHP Plan
SLUCare UHC In-Network Out-of-Network SLUCare UHC In-Network Out-of-Network
Deductible Non-Embedded:
Individual $0 $500 $750 $1,500 $1,500 $3,000
Family $0 $1,000 $1,500 $3,000 $3,000 $6,000
Coinsurance 0% 10% 40% 0% 10% 40%
Out-of-Pocket Maximum (includes deductibles and copays) Non-Embedded:
Individual $1,500 $1,500 $4,750 $1,500 $3,000 $6,000
Family $3,000 $3,000 $9,500 $3,000 $6,000 $12,000
Physician Ofice Visits
Primary Care $10 copay 10% after ded. 40% after ded. 0% after ded. 10% after ded. 40% after ded.
Specialist Care $20 copay 10% after ded. 40% after ded. 0% after ded. 10% after ded. 40% after ded.
Inpatient Hospital
N/A 10% after ded. 40% after ded. N/A 10% after ded. 40% after ded.
Emergency Room
N/A $100 copay $100 copay N/A 10% after ded. 10% after ded.
Urgent Care Center
N/A $50 copay 40% after ded. N/A 10% after ded. 40% after ded.
Plus Plan QHDHP Plan
Retail (34-day supply) Mail Order (90-day supply) Retail (34-day supply) Mail Order (90-day supply)
Tier 1 $8 $16 Medical Deductible and Coinsurance
Tier 2 $30 $60 Medical Deductible and Coinsurance
Tier 3 $50 $100 Medical Deductible and Coinsurance
Tier 4 20% to $150 Not covered Medical Deductible and Coinsurance
Select Preventive Priced according to the tier in which they fall Covered at 100%, no copay or deductible
Medications
Dental Plan Comparison
Schedule of Beneits Flex Option Basic Plus Option
Type of Plan Delta Dental PPO Delta Dental PPO
Network Considerations In PPO Network Out of PPO Network * In PPO Network Out of PPO Network *
Coinsurance (Plan Pays)
Type A: Preventive Care 100% 100% 100% 50%
Type B: Basic Restorative Services 90% 70% 70% 35%
Type C: Major Restorative Services 60% 40% 40% 20%
Type D: Orthodontics 50% 40% 50% 25%
Deductible (Applies to) B & C Services B & C Services B & C Services B & C Services
Per Person $50 $50 $25 $25
Per Family $150 $150 $75 $75
Beneit Maximums
Annual Beneit Maximum Per Person $1,500 $1,500 $1,000 $1,000
Lifetime Orthodontia Beneit Maximum $1,000 adult and $1,000 adult and child $1,000 child only $1,000 child only
child (up to age 26) (up to age 26) (up to age 19) (up to age 19)
* Delta Premier Network or non-participating providers
6