
Page 55 - Tampa Bay Rays 2022 Flipbook
P. 55
*
If
Self
Child
Other
Child
Other
Child
Child
Other
Other
Child
Child
Other
Other
Spouse
Complete
Applicable
Mailing Address
Required for
Dom. Part.
Change of Name
Change of Phone
Employer/Group Name
Change of Address
Employee Phone Number
Employee (Member) Identification Number
all members/dependents
Change Birthdate
Change Effective Date
Employee (Member) First Name / Middle Initial / Last Name
New
Existing
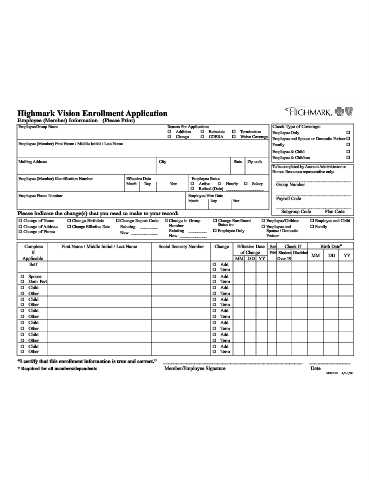
Employee (Member) Information (Please Print)
Month
First Name / Middle Initial / Last Name
Effective Date
Day
____________
________
Change Report Code
“I certify that this enrollment information is true and correct.”
City
Highmark Vision Enrollment Application
New
Year
Please indicate the change(s) that you need to make to your record:
Number
Existing
Change
Addition
Month
Change in Group
Social Security Number
____________
________
Reason For Application:
Active
Day
Employee Status
COBRA
Employee Hire Date
Retired (Date)
Reinstate
Member/Employee Signature
Add
Add
Add
Add
Add
Add
Add
Add
Change
Term
Term
Term
Term
Term
Term
Term
Term
Status to:
Hourly
Year
State
Employee Only
Change Enrollment
Termination
of Change
Zip code
Salary
__________________
Effective Date
MM DD YY
Waive Coverage
F/M
Sex
Partner
Family
Student
Over 19
Employee and
Employee &
Employee &
Spouse / Domestic
Employee/Children
Employee Only
Payroll Code
Check If
______________________________________________________
Group Number
Child
Disabled
Subgroup Code
Children
MM
Check Type of Coverage:
Date
Family
DD
Human Resources representative only:
Birth Date*
Plan Code
Employee and Spouse or Domestic Partner
To be completed by Account Administrator or
Employee and Child
YY
________________
________________________________
________________________________
________________________________
MS00109 4/10/08