
Page 6 - University of the South-2022-Benefit Guide REVISED 3.30.22 FSA WAIT PERIOD
P. 6
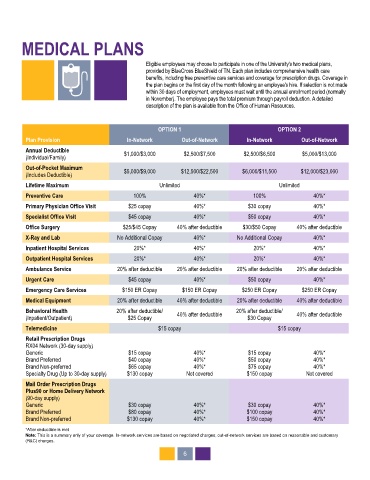
MEDICAL PLANS
Eligible employees may choose to participate in one of the University's two medical plans,
provided by BlueCross BlueShield of TN. Each plan includes comprehensive health care
benefits, including free preventive care services and coverage for prescription drugs. Coverage in
the plan begins on the first day of the month following an employee's hire. If selection is not made
within 30 days of employment, employees must wait until the annual enrollment period (normally
in November). The employee pays the total premium through payroll deduction. A detailed
description of the plan is available from the Office of Human Resources.
OPTION 1 OPTION 2
Plan Provision In-Network Out-of-Network In-Network Out-of-Network
Annual Deductible $1,000/$3,000 $2,500/$7,500 $2,500/$6,500 $5,000/$13,000
(Individual/Family)
Out-of-Pocket Maximum $5,000/$9,000 $12,500/$22,500 $6,000/$11,500 $12,000/$23,000
(Includes Deductible)
Lifetime Maximum Unlimited Unlimited
Preventive Care 100% 40%* 100% 40%*
Primary Physician Office Visit $25 copay 40%* $30 copay 40%*
Specialist Office Visit $45 copay 40%* $50 copay 40%*
Office Surgery $25/$45 Copay 40% after deductible $30/$50 Copay 40% after deductible
X-Ray and Lab No Additional Copay 40%* No Additional Copay 40%*
Inpatient Hospital Services 20%* 40%* 20%* 40%*
Outpatient Hospital Services 20%* 40%* 20%* 40%*
Ambulance Service 20% after deductible 20% after deductible 20% after deductible 20% after deductible
Urgent Care $45 copay 40%* $50 copay 40%*
Emergency Care Services $150 ER Copay $150 ER Copay $250 ER Copay $250 ER Copay
Medical Equipment 20% after deductible 40% after deductible 20% after deductible 40% after deductible
Behavioral Health 20% after deductible/ 40% after deductible 20% after deductible/ 40% after deductible
(Inpatient/Outpatient) $25 Copay $30 Copay
Telemedicine $15 copay $15 copay
Retail Prescription Drugs
RX04 Network (30-day supply)
Generic $15 copay 40%* $15 copay 40%*
Brand Preferred $40 copay 40%* $50 copay 40%*
Brand Non-preferred $65 copay 40%* $75 copay 40%*
Specialty Drug (Up to 30-day supply) $130 copay Not covered $150 copay Not covered
Mail Order Prescription Drugs
Plus90 or Home Delivery Network
(90-day supply)
Generic $30 copay 40%* $30 copay 40%*
Brand Preferred $80 copay 40%* $100 copay 40%*
Brand Non-preferred $130 copay 40%* $150 copay 40%*
*After deductible is met
Note: This is a summary only of your coverage. In-network services are based on negotiated charges; out-of-network services are based on reasonable and customary
(R&C) charges.
6