
Page 686 - outbind://23/
P. 686
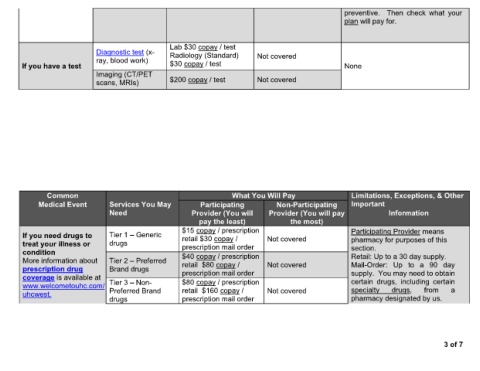
preventive. Then check what your
plan will pay for.
Lab $30 copay / test
Diagnostic test (x- Radiology (Standard) Not covered
ray, blood work)
If you have a test $30 copay / test None
Imaging (CT/PET
scans, MRIs) $200 copay / test Not covered
Common What You Will Pay Limitations, Exceptions, & Other
Medical Event Services You May Participating Non-Participating Important
Need Provider (You will Provider (You will pay Information
pay the least) the most)
$15 copay / prescription Participating Provider means
If you need drugs to Tier 1 Generic retail $30 copay / Not covered pharmacy for purposes of this
treat your illness or drugs prescription mail order
condition $40 copay / prescription section.
Retail: Up to a 30 day supply.
More information about Tier 2 Preferred retail $80 copay / Not covered Mail-Order: Up to a 90 day
prescription drug Brand drugs prescription mail order supply. You may need to obtain
coverage is available at certain drugs, including certain
www.welcometouhc.com/ Tier 3 Non- $80 copay / prescription
uhcwest. Preferred Brand retail $160 copay / Not covered specialty drugs, from a
drugs prescription mail order pharmacy designated by us.
3 of 7