
Page 688 - outbind://23/
P. 688
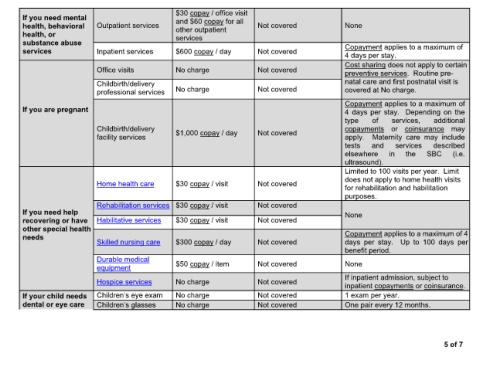
$30 copay / office visit
If you need mental and $60 copay for all
health, behavioral Outpatient services other outpatient Not covered None
health, or services
substance abuse Copayment applies to a maximum of
services Inpatient services $600 copay / day Not covered
4 days per stay.
Cost sharing does not apply to certain
Office visits No charge Not covered
preventive services. Routine pre-
Childbirth/delivery natal care and first postnatal visit is
professional services No charge Not covered covered at No charge.
Copayment applies to a maximum of
If you are pregnant 4 days per stay. Depending on the
type of services, additional
Childbirth/delivery $1,000 copay / day Not covered copayments or coinsurance may
facility services apply. Maternity care may include
tests and services described
elsewhere in the SBC (i.e.
ultrasound).
Limited to 100 visits per year. Limit
does not apply to home health visits
Home health care $30 copay / visit Not covered
for rehabilitation and habilitation
purposes.
Rehabilitation services $30 copay / visit Not covered
If you need help None
recovering or have Habilitative services $30 copay / visit Not covered
other special health
needs Copayment applies to a maximum of 4
Skilled nursing care $300 copay / day Not covered days per stay. Up to 100 days per
benefit period.
Durable medical
equipment $50 copay / item Not covered None
If inpatient admission, subject to
Hospice services No charge Not covered
inpatient copayments or coinsurance.
If your child needs No charge Not covered 1 exam per year.
dental or eye care No charge Not covered One pair every 12 months.
5 of 7