
Page 771 - outbind://23/
P. 771
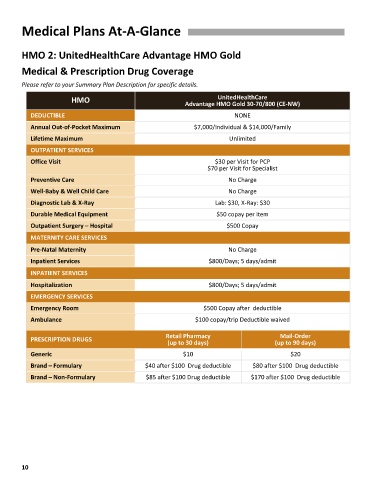
Medical Plans At-A-Glance
HMO 2: UnitedHealthCare Advantage HMO Gold
Medical & Prescription Drug Coverage
Please refer to your Summary Plan Description for specific details.
UnitedHealthCare
HMO Advantage HMO Gold 30-70/800 (CE-NW)
DEDUCTIBLE NONE
Annual Out-of-Pocket Maximum $7,000/Individual & $14,000/Family
Lifetime Maximum Unlimited
OUTPATIENT SERVICES
Office Visit $30 per Visit for PCP
$70 per Visit for Specialist
Preventive Care No Charge
Well-Baby & Well Child Care No Charge
Diagnostic Lab & X-Ray Lab: $30, X-Ray: $30
Durable Medical Equipment $50 copay per item
Outpatient Surgery – Hospital $500 Copay
MATERNITY CARE SERVICES
Pre-Natal Maternity No Charge
Inpatient Services $800/Days; 5 days/admit
INPATIENT SERVICES
Hospitalization $800/Days; 5 days/admit
EMERGENCY SERVICES
Emergency Room $500 Copay after deductible
Ambulance $100 copay/trip Deductible waived
Mail-Order
PRESCRIPTION DRUGS Retail Pharmacy (up to 90 days)
(up to 30 days)
Generic $10 $20
Brand – Formulary $40 after $100 Drug deductible $80 after $100 Drug deductible
Brand – Non-Formulary $85 after $100 Drug deductible $170 after $100 Drug deductible
10