
Page 5 - Microsoft Word - CNLV Benefits Booklet Draft Revised 10.31.19 NON RETIREE.docx
P. 5
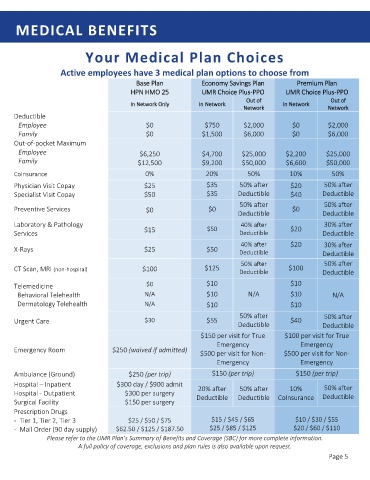
MEDICAL BENEFITS
Your Medical Plan Choices
Active employees have 3 medical plan options to choose from
E
Economy Savings Plconomy Savings Planan
Base PlanBase Plan
Base Planase Plan
Premium Planremium Plan
Premium PlanPremium Plan
B Economy Savings PlEconomy Savings Planan P
HPNHPN HMO 25HMO 25 U UU UMRMR Choice PlusChoice Plus--PPOPPO U UU UMRMR Choice PlusChoice Plus--PPOPPO
H
HPNPN HMO 25HMO 25
MRMR Choice PlusChoice Plus--PPOPPO
MRMR Choice PlusChoice Plus--PPOPPO
Out of ut of
Out of ut of
O O
Out of Out of
Out of Out of
I
I
In Network Onlyn Network Only In Networkn Network I In Networkn Network
In NetworkIn Network
In NetworkIn Network
In Network OnlyIn Network Only
Networketwork N
NetworkNetwork
NetworkNetwork
N
Networketwork
Deductible
Employee $0 $750 $2,000 $0 $2,000
Family $0 $1,500 $6,000 $0 $6,000
Out-of-pocket Maximum
Employee $6,250 $4,700 $25,000 $2,200 $25,000
Family $12,500 $9,200 $50,000 $6,600 $50,000
CoInsurance 0% 20% 50% 10% 50%
Physician Visit Copay $25 $35 50% after $20 50% after
Specialist Visit Copay $50 $35 Deductible $40 Deductible
50% after 50% after
Preventive Services $0 $0 $0
Deductible Deductible
Laboratory & Pathology 40% after 30% after
$15 $50 $20
Services Deductible Deductible
40% after $20 30% after
X-Rays $25 $50
Deductible Deductible
50% after 50% after
CT Scan, MRI (non-hospital) $100 $125 $100
Deductible Deductible
Telemedicine $0 $10 $10
Behavioral Telehealth N/A $10 N/A $10 N/A
Dermatology Telehealth N/A $10 $10
50% after 50% after
Urgent Care $30 $55 $40
Deductible Deductible
$150 per visit for True $100 per visit for True
Emergency Emergency
Emergency Room $250 (waived if admitted)
$500 per visit for Non- $500 per visit for Non-
Emergency Emergency
Ambulance (Ground) $250 (per trip) $150 (per trip) $150 (per trip)
Hospital – Inpatient $300 day / $900 admit
20% after 50% after 10% 50% after
Hospital - Outpatient $300 per surgery Deductible CoInsurance Deductible
Surgical Facility $150 per surgery Deductible
Prescription Drugs
- Tier 1, Tier 2, Tier 3 $25 / $50 / $75 $15 / $45 / $65 $10 / $30 / $55
- Mail Order (90 day supply) $62.50 / $125 / $187.50 $25 / $85 / $125 $20 / $60 / $110
Please refer to the UMR Plan’s Summary of Benefits and Coverage (SBC) for more complete information.
A full policy of coverage, exclusions and plan rules is also available upon request.
Page 5