
Page 12 - Omega Benefits Guide
P. 12
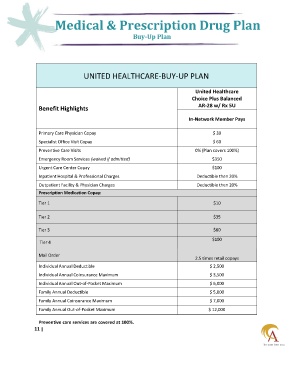
Medical & Prescription Drug Plan
Buy-Up Plan
UNITED HEALTHCARE-BUY-UP PLAN
United Healthcare
Choice Plus Balanced
AR-28 w/ Rx 5U
Benefit Highlights
In-Network Member Pays
Primary Care Physician Copay $ 30
Specialist Office Visit Copay $ 60
Preventive Care Visits 0% (Plan covers 100%)
Emergency Room Services (waived if admitted) $350
Urgent Care Center Copay $100
Inpatient Hospital & Professional Charges Deductible then 20%
Outpatient Facility & Physician Charges Deductible then 20%
Prescription Medication Copay:
Tier 1 $10
Tier 2 $35
Tier 3 $60
$100
Tier 4
Mail Order
2.5 times retail copays
Individual Annual Deductible $ 2,500
Individual Annual Coinsurance Maximum $ 3,500
Individual Annual Out-of-Pocket Maximum $ 6,000
Family Annual Deductible $ 5,000
Family Annual Coinsurance Maximum $ 7,000
Family Annual Out-of-Pocket Maximum $ 12,000
Preventive care services are covered at 100%.
11 |