
Page 11 - Allegacy 2019 Benefit Guide Part Time
P. 11
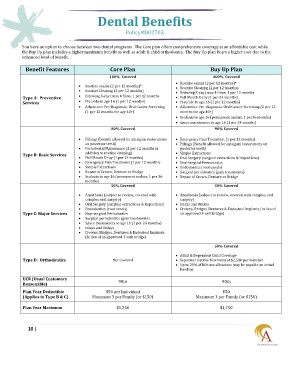
Dental Benefits
Policy#D02703
You have an option to choose between two dental programs. The Core plan offers comprehensive coverage at an affordable cost while
the Buy Up plan includes a higher maximum benefit as well as adult & child orthodontia. The Buy Up plan bears a higher cost due to the
enhanced level of benefit.
Benefit Features Core Plan Buy Up Plan
100% Covered 100% Covered
Routine exams (2 per 12 months)*
Routine exams (2 per 12 months)* Routine Cleaning (2 per 12 months)
Routine Cleaning (2 per 12 months) Bitewing X-ray (max 4 films; 1 per 12 months
Type A: Preventive Bitewing X-ray (max 4 films; 1 per 12 months Full Mouth X-ray (1 per 24 months)
Services Fluoride to age 16 (1 per 12 months) Fluoride to age 16 (1 per 12 months)
Adjunctive Pre-Diagnostic Oral Cancer Screening Adjunctive Pre-Diagnostic Oral Cancer Screening (1 per 12
(1 per 12 months for age 40+) months for age 40+)
Sealants to age 16 (permanent molars, 1 per36 months)
Space maintainers to age 16 (1 per 24 months)
80% Covered 90% Covered
Fillings (benefit allowed for amalgam restorations Emergency Pain Treatment (1 per 12 months)
on posterior teeth) Fillings (Benefit allowed for amalgam restorations on
Periodontal Mainenance (2 per 12 months in posterior teeth)
Type B: Basic Services addition to routine cleaning) Simple Extractions
Full Mouth X-ray (1 per 24 months) Oral Surgery (surgical extractions & impactions)
Emergency Pain Treatment (1 per 12 months) Non-surgical Periodontics
Simple Extractions Endodontics (root canals)
Repair of Crown, Denture or Bridge Surgical periodontics (gum treatments)
Sealants to age 16 (permanent molars, 1 per 36 Repair of Crown, Denture or Bridge
months)
50% Covered 50% Covered
Anesthesia (subject to review, covered with Anesthesia (subject to review, covered with complex oral
complex oral surgery) surgery)
Oral Surgery (surgical extractions & impactions) Inlays and Onlays
Endodontics (root canals) Crowns, Bridges, Dentures & Endosteal Implants (in lieu of
Type C: Major Services Non-surgical Periodontics an approved 3-unit bridge)
Surgical periodontics (gum treatments)
Space maintainers to age 16 (1 per 24 months)
Inlays and Onlays
Crowns, Bridges, Dentures & Endosteal Implants
(in lieu of an approved 3-unit bridge)
50% Covered
Adult & Dependent Child Coverage
Type D: Orthodontics Not Covered Separate Lifetime Maximum of $2,500 per member
Up to 25% of lifetime allowance may be payable on initial
banding
UCR (Usual Customary 90th 90th
Reasonable)
Plan Year Deductible $50 per Individual $50
(Applies to Type B & C) Maximum 3 per Family (or $150) Maximum 3 per Family (or $150)
Plan Year Maximum $1,250 $1,750
10 |