
Page 5 - 2018 Endeavor Schools Benefit Guide
P. 5
3
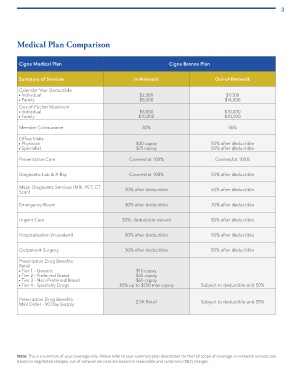
Medical Plan Comparison
Cigna Medical Plan Cigna Bronze Plan
Summary of Services In-Network Out-of-Network
Calendar Year Deductible
Individual $2,500 $7,000
Family $5,000 $14,000
Out-of-Pocket Maximum
Individual $5,000 $10,000
Family $10,000 $20,000
Member Coinsurance 30% 50%
Office Visits
Physician $30 copay 50% after deductible
Specialist $75 copay 50% after deductible
Preventative Care Covered at 100% Covered at 100%
Diagnostic Lab & X-Ray Covered at 100% 50% after deductible
Major Diagnostic Services (MRI, PET, CT 30% after deductible 50% after deductible
Scan)
Emergency Room 30% after deductible 30% after deductible
Urgent Care 30%; deductible waived 50% after deductible
Hospitalization (In-patient) 30% after deductible 50% after deductible
Outpatient Surgery 30% after deductible 50% after deductible
Prescription Drug Benefits
Retail
Tier 1 - Generic $15 copay
Tier 2 - Preferred Brand $35 copay
Tier 3 - Non-Preferred Brand $65 copay
Tier 4 - Specialty Drugs 30% up to $250 max copay Subject to deductible and 50%
Prescription Drug Benefits 2.5X Retail Subject to deductible and 50%
Mail Order - 90 Day Supply
Note: This is a summary of your coverage only. Please refer to your summary plan description for the full scope of coverage. In-network services are
based on negotiated charges; out-of-network services are based on reasonable and customary (R&C) charges.