
Page 19 - 2021_Gray West_Benefits_Guide_Final
P. 19
Quick Contact Details:
Your Health Phone: 866-723-0515
Website: anthem.com
Anthem Blue Login to your Anthem
account at anthem.com
View Vision Download Mobile Health in the
App Store or Google Play
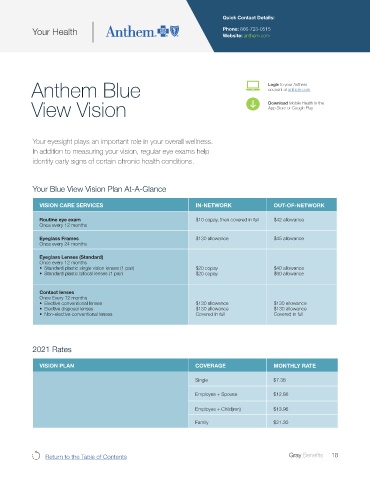
Your eyesight plays an important role in your overall wellness.
In addition to measuring your vision, regular eye exams help
identify early signs of certain chronic health conditions.
Your Blue View Vision Plan At-A-Glance
VISION CARE SERVICES IN-NETWORK OUT-OF-NETWORK
Routine eye exam $10 copay, then covered in full $42 allowance
Once every 12 months
Eyeglass Frames $130 allowance $45 allowance
Once every 24 months
Eyeglass Lenses (Standard)
Once every 12 months
• Standard plastic single vision lenses (1 pair) $20 copay $40 allowance
• Standard plastic bifocal lenses (1 pair) $20 copay $60 allowance
Contact lenses
Once Every 12 months
• Elective conventional lenses $130 allowance $130 allowance
• Elective disposal lenses $130 allowance $130 allowance
• Non-elective conventional lenses Covered in full Covered in full
2021 Rates
VISION PLAN COVERAGE MONTHLY RATE
Single $7.36
Employee + Spouse $12.86
Employee + Child(ren) $13.96
Family $21.30
Return to the Table of Contents Gray Benefits 18