
Page 27 - USUI Benefit Book
P. 27
3 of 8
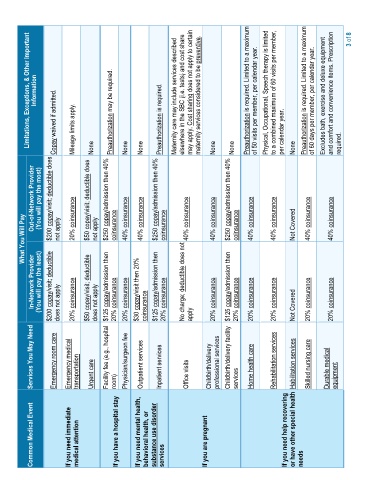
Information Limitations, Exceptions, & Other Important Maternity care may include services described elsewhere in the SBC (i.e. tests) and cost share may apply. Cost sharing does not apply to certain maternity services considered to be preventive. Preauthorization is required. Limited to a maximum of 50 visits per member, per calendar year. Physical, Occupational, Speech therapy is limited to a combined maximum of 60 visits per member, Preauthorization is
Mileage limits apply. None Preauthorization may be required. None None Preauthorization is required. None None per calendar year. None required.
Out-of-Network Provider (You will pay the most) $200 copay/visit; deductible does Copay waived if admitted. 20% coinsurance $50 copay/visit; deductible does $250 copay/admission then 40% 40% coinsurance $250 copay/admission then 40% $250 copay/admission then 40% 40% coinsurance 40% coinsurance 40% coinsurance 40% coinsurance
What You Will Pay not apply not apply coinsurance 40% coinsurance coinsurance No charge; deductible does not 40% coinsurance 40% coinsurance coinsurance Not Covered
In-Network Provider (You will pay the least) $200 copay/visit; deductible does not apply 20% coinsurance $50 copay/visit; deductible does not apply $125 copay/admission then 20% coinsurance 20% coinsurance $30 copay/visit then 20% coinsurance $125 copay/admission then 20% coinsurance apply 20% coinsurance $125 copay/admission then 20% coinsurance 20% coinsurance 20% coinsurance Not Covered 20% coinsurance 20% coinsura
Services You May Need Emergency room care Emergency medical transportation Urgent care Facility fee (e.g., hospital room) Physician/surgeon fee Outpatient services Inpatient services Office visits Childbirth/delivery professional services Childbirth/delivery facility services Home health care Rehabilitation services Habilitation services Skilled nursing care Durable medical equipment
Common Medical Event If you need immediate medical attention If you have a hospital stay If you need mental health, behavioral health, or substance use disorder services If you are pregnant If you need help recovering or have other special health needs