
Page 28 - USUI Benefit Book
P. 28
4 of 8
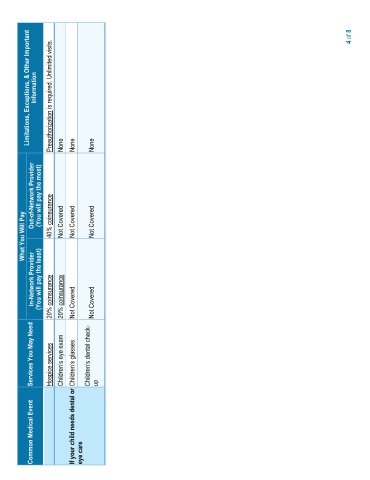
Information Limitations, Exceptions, & Other Important Preauthorization is required. Unlimited visits.
None None None
Out-of-Network Provider (You will pay the most) 40% coinsurance
What You Will Pay Not Covered Not Covered Not Covered
In-Network Provider (You will pay the least) 20% coinsurance 20% coinsurance Not Covered Not Covered
Services You May Need Hospice services dental check- up
Common Medical Event If your child needs dental or eye care