
Page 4 - Forms - New Patient Paperwork (Dec-2017)_Neat
P. 4
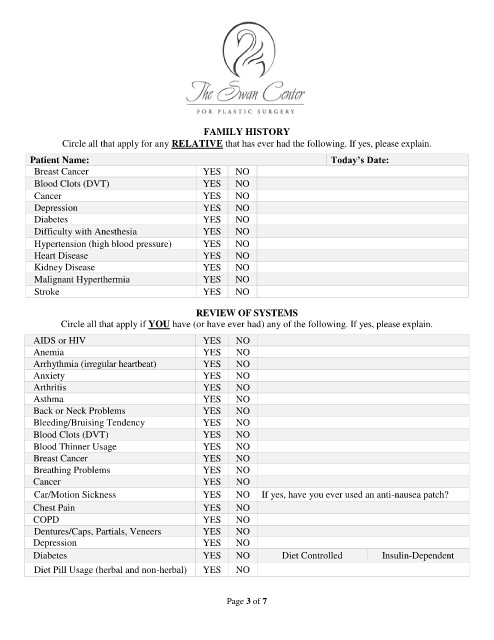
FAMILY HISTORY
Circle all that apply for any RELATIVE that has ever had the following. If yes, please explain.
Patient Name: Today’s Date:
Breast Cancer YES NO
Blood Clots (DVT) YES NO
Cancer YES NO
Depression YES NO
Diabetes YES NO
Difficulty with Anesthesia YES NO
Hypertension (high blood pressure) YES NO
Heart Disease YES NO
Kidney Disease YES NO
Malignant Hyperthermia YES NO
Stroke YES NO
REVIEW OF SYSTEMS
Circle all that apply if YOU have (or have ever had) any of the following. If yes, please explain.
AIDS or HIV YES NO
Anemia YES NO
Arrhythmia (irregular heartbeat) YES NO
Anxiety YES NO
Arthritis YES NO
Asthma YES NO
Back or Neck Problems YES NO
Bleeding/Bruising Tendency YES NO
Blood Clots (DVT) YES NO
Blood Thinner Usage YES NO
Breast Cancer YES NO
Breathing Problems YES NO
Cancer YES NO
Car/Motion Sickness YES NO If yes, have you ever used an anti-nausea patch?
Chest Pain YES NO
COPD YES NO
Dentures/Caps, Partials, Veneers YES NO
Depression YES NO
Diabetes YES NO Diet Controlled Insulin-Dependent
Diet Pill Usage (herbal and non-herbal) YES NO
Page 3 of 7