
Page 140 - Business Development Orientation Binder
P. 140
Patient Name __________________________________________________ Date of Birth_______/________/________
VNSNY MRN ___________________________________________________ Case No _____________________________
Hospital/Institution______________________________________________ Record_______________________________
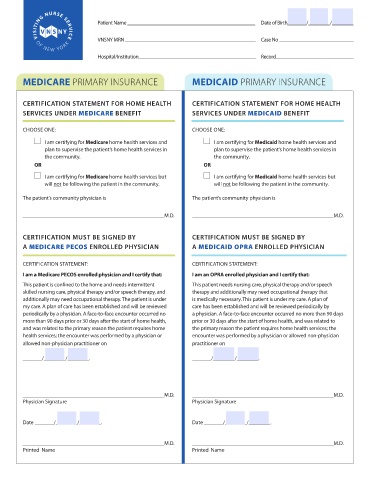
MEDICARE PRIMARY INSURANCE MEDICAID PRIMARY INSURANCE
CERTIFICATION STATEMENT FOR HOME HEALTH CERTIFICATION STATEMENT FOR HOME HEALTH
SERVICES UNDER MEDICARE BENEFIT SERVICES UNDER MEDICAID BENEFIT
CHOOSE ONE: CHOOSE ONE:
I am certifying for Medicare home health services and I am certifying for Medicaid home health services and
plan to supervise the patient’s home health services in plan to supervise the patient’s home health services in
the community. the community.
OR OR
I am certifying for Medicare home health services but I am certifying for Medicaid home health services but
will not be following the patient in the community. will not be following the patient in the community.
The patient’s community physician is The patient’s community physician is
____________________________________________________M.D. ____________________________________________________M.D.
CERTIFICATION MUST BE SIGNED BY CERTIFICATION MUST BE SIGNED BY
A MEDICARE PECOS ENROLLED PHYSICIAN A MEDICAID OPRA ENROLLED PHYSICIAN
CERTIFICATION STATEMENT: CERTIFICATION STATEMENT:
I am a Medicare PECOS enrolled physician and I certify that: I am an OPRA enrolled physician and I certify that:
This patient is confined to the home and needs intermittent This patient needs nursing care, physical therapy and/or speech
skilled nursing care, physical therapy and/or speech therapy, and therapy and additionally may need occupational therapy that
additionally may need occupational therapy. The patient is under is medically necessary. This patient is under my care. A plan of
my care. A plan of care has been established and will be reviewed care has been established and will be reviewed periodically by
periodically by a physician. A face-to-face encounter occurred no a physician. A face-to-face encounter occurred no more than 90 days
more than 90 days prior or 30 days after the start of home health, prior or 30 days after the start of home health, and was related to
and was related to the primary reason the patient requires home the primary reason the patient requires home health services; the
health services; the encounter was performed by a physician or encounter was performed by a physician or allowed non-physician
allowed non-physician practitioner on practitioner on
_______/________/________. _______/________/________.
____________________________________________________M.D. ____________________________________________________M.D.
Physician Signature Physician Signature
Date _______/________/________. Date _______/________/________.
____________________________________________________M.D. ____________________________________________________M.D.
Printed Name Printed Name