
Page 674 - Equine Clinical Medicine, Surgery and Reproduction, 2nd Edition
P. 674
Respir atory system: 3.2 Surgical conditions of the respir atory tr act 649
VetBooks.ir with pronounced vasculature. In an entrapment the the standing sedated horse. The pharynx is anaes-
thetised using topical lidocaine or mepivicaine
epiglottis is present (unless there is a secondary dis-
placed soft palate) but will present with a smooth
knife is then passed via the contralateral nostril and
edge and no vasculature due to the covering mucosa. delivered by the endoscope. A custom-built hook
The coverage of the epiglottis is variable. In long- used to hook the entrapping membrane. The knife
standing cases the caudal edge of the entrapment is then progressively withdrawn until the mem-
may become ulcerated and, occasionally, the apex brane is transected down the midline. The entrap-
of the epiglottis may erode through the entrapment ping membrane is tough and considerable traction
(Fig. 3.93). Intermittent entrapments are more of is necessary to transect it. Great care is necessary
a diagnostic challenge. Almost all entrapments are to ensure no trauma occurs to other pharyngeal
precipitated by deglutition, not by exercise, and structures, particularly the soft palate. Guarded
therefore careful assessment of several deglutition or closed hook knives are now available that limit
sequences is indicated. Dynamic endoscopy is rarely the risks of this procedure. The entrapped mucosa
necessary for diagnosis as most cases can be diag- can also be incised via a transendoscopic laser fol-
nosed at rest. Radiography of the pharynx can reveal lowing topical local anaesthesia. However, thermal
the blunted outline of an entrapped epiglottis, epi- damage to the epiglottis can result as the plane of
glottic hypoplasia and subepiglottic cysts. dissection is orthogonal to the endoscopic view.
Due to the risks of iatrogenic palatal trauma and
Management the limitation of stable entrapments only, many
Intermittent cases can be managed successfully by authors prefer to perform the procedure under
anti-inflammatory medication. Medication is usually general anaesthesia (Fig. 3.94). The same hook
administered as a nasal spray using a canine urinary knife can be used, passed via the mouth, under oral
catheter. A combination of DMSO, hydrocortisone endoscopic examination. In those cases where tran-
and propylene glycol is often used. secting the entrapping membrane does not release
Most cases of epiglottic entrapment are managed the entrapment, resection via a laryngotomy is
surgically. Stable entrapments can be managed in necessary.
3.93 3.94
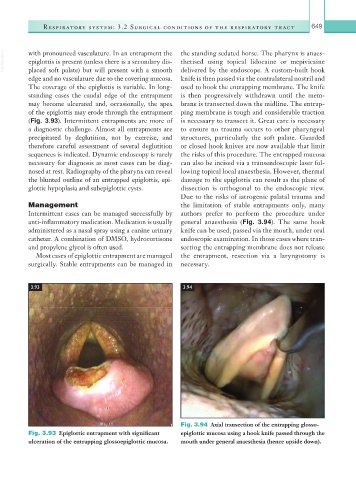
Fig. 3.94 Axial transection of the entrapping glosso-
Fig. 3.93 Epiglottic entrapment with significant epiglottic mucosa using a hook knife passed through the
ulceration of the entrapping glossoepiglottic mucosa. mouth under general anaesthesia (hence upside down).