
Page 142 - Clinical Pearls in Cardiology
P. 142
130 Clinical Pearls in Cardiology
2. Due to fastidious organisms (e.g. HACEK group)
3. Intracellular bacteria like Coxiella burnetii, Chlamydia
or Tropheryma whipplei
4. Marantic or nonbacterial thrombotic endocarditis
(seen in metastatic cancer)
5. Libman-Sacks or nonbacterial verrucous endocarditis
(seen in SLE).
4. Which are the clinical situations that warrant the
suspicion of infective endocarditis?
Infective endocarditis should be suspected in a variety
of very different clinical situations like the following:
1. New regurgitant cardiac murmur
2. Embolic events of unknown origin
3. Sepsis of unknown origin
4. Prolonged unexplained fever.
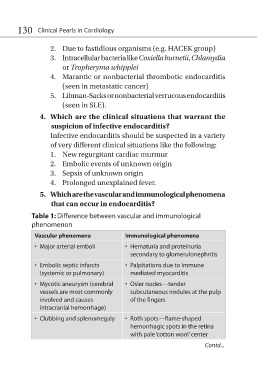
5. Which are the vascular and immunological phenomena
that can occur in endocarditis?
Table 1: Difference between vascular and immunological
phenomenon
Vascular phenomena Immunological phenomena
• Major arterial emboli • Hematuria and proteinuria
secondary to glomerulonephritis
• Embolic septic infarcts • Palpitations due to immune
(systemic or pulmonary) mediated myocarditis
• Mycotic aneurysm (cerebral • Osler nodes—tender
vessels are most commonly subcutaneous nodules at the pulp
involved and causes of the fingers
intracranial hemorrhage)
• Clubbing and splenomegaly • Roth spots—flame-shaped
hemorrhagic spots in the retina
with pale ‘cotton wool’ center
Contd...