
Page 79 - Clinical Pearls in Cardiology
P. 79
Jugular Venous Pulse 67
Contd...
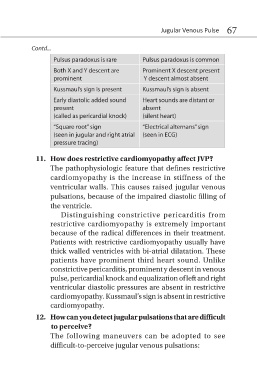
Pulsus paradoxus is rare Pulsus paradoxus is common
Both X and Y descent are Prominent X descent present
prominent Y descent almost absent
Kussmaul’s sign is present Kussmaul’s sign is absent
Early diastolic added sound Heart sounds are distant or
present absent
(called as pericardial knock) (silent heart)
“Square root” sign “Electrical alternans” sign
(seen in jugular and right atrial (seen in ECG)
pressure tracing)
11. How does restrictive cardiomyopathy affect JVP?
The pathophysiologic feature that defines restrictive
cardiomyopathy is the increase in stiffness of the
ventricular walls. This causes raised jugular venous
pulsations, because of the impaired diastolic filling of
the ventricle.
Distinguishing constrictive pericarditis from
restrictive cardiomyopathy is extremely important
because of the radical differences in their treatment.
Patients with restrictive cardiomyopathy usually have
thick walled ventricles with bi-atrial dilatation. These
patients have prominent third heart sound. Unlike
constrictive pericarditis, prominent y descent in venous
pulse, pericardial knock and equalization of left and right
ventricular diastolic pressures are absent in restrictive
cardiomyopathy. Kussmaul’s sign is absent in restrictive
cardiomyopathy.
12. How can you detect jugular pulsations that are difficult
to perceive?
The following maneuvers can be adopted to see
difficult-to-perceive jugular venous pulsations: