
Page 60 - On Call folder
P. 60
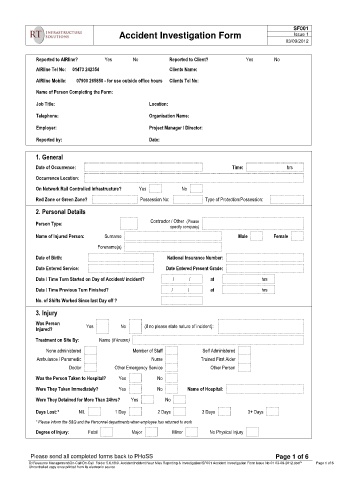
SF001
Accident Investigation Form Issue 1
03/09/2012
Reported to AIRline? Yes No Reported to Client? Yes No
AIRline Tel No: 01473 242354 Clients Name:
AIRline Mobile: 07900 265850 - for use outside office hours Clients Tel No:
Name of Person Completing the Form:
Job Title: Location:
Telephone: Organisation Name:
Employer: Project Manager / Director:
Reported by: Date:
1. General
Date of Occurrence: Time: hrs
Occurrence Location:
On Network Rail Controlled Infrastructure? Yes No
Red Zone or Green Zone? Possession No: Type of Protection/Possession:
2. Personal Details
Contractor / Other (Please
Person Type: specify company)
Name of Injured Person: Surname Male Female
Forename(s)
Date of Birth: National Insurance Number:
Date Entered Service: Date Entered Present Grade:
Date / Time Turn Started on Day of Accident/ incident? / / at hrs
Date / Time Previous Turn Finished? / / at hrs
No. of Shifts Worked Since last Day off ?
3. Injury
Was Person
Yes No (if no please state nature of incident):
Injured?
Treatment on Site By: Name (if known)
None administered Member of Staff Self Administered
Ambulance / Paramedic Nurse Trained First Aider
Doctor Other Emergency Service Other Person
Was the Person Taken to Hospital? Yes No
Were They Taken Immediately? Yes No Name of Hospital:
Were They Detained for More Than 24hrs? Yes No
Days Lost:* NIL 1 Day 2 Days 3 Days 3+ Days
* Please inform the S&Q and the Personnel departments when employee has returned to work
Degree of Injury: Fatal Major Minor No Physical Injury
Page 1 of 6
Please send all completed forms back to PHoSS Page 1 of 6
S:\Resource Management\On-Call\On-Call Folder 5.6.18\9. AccidentIncident Near Miss Reporting & Investigation\SF001 Accident Investigation Form Issue No 01 03-09-2012.docP Page 1 of 6
Uncontrolled copy once printed from its electronic source