
Page 11 - 11639_2019 Open EnrollmentGuidebook_interactive
P. 11
MY HEALTH
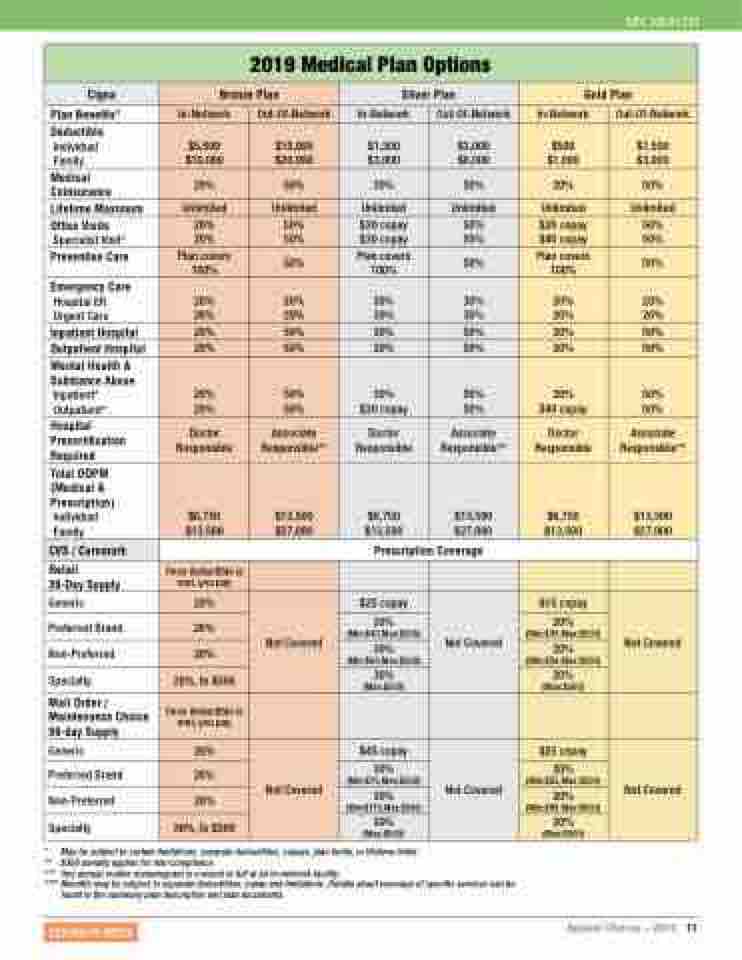
2019 Medical Plan Options
Cigna
Bronze Plan
Silver Plan
Gold Plan
Plan Benefits*
In-Network
Out-Of-Network
In-Network
Out-Of-Network
In-Network
Out-Of-Network
Deductible
Individual Family
$5,000 $10,000
$10,000 $20,000
$1,500 $3,000
$3,000 $6,000
$500 $1,000
$1,500 $3,000
Medical Coinsurance
20%
50%
30%
50%
20%
50%
Lifetime Maximum
Unlimited
Unlimited
Unlimited
Unlimited
Unlimited
Unlimited
Office Visits
Specialist Visit*
20% 20%
50% 50%
$30 copay $30 copay
50% 50%
$20 copay $40 copay
50% 50%
Preventive Care
Plan covers 100%
50%
Plan covers 100%
50%
Plan covers 100%
50%
Emergency Care
Hospital ER Urgent Care
20% 20%
20% 20%
30% 30%
30% 30%
20% 20%
20% 20%
Inpatient Hospital
20%
50%
30%
50%
20%
50%
Outpatient Hospital
20%
50%
30%
50%
20%
50%
Mental Health & Substance Abuse
Inpatient* Outpatient*
20% 20%
50% 50%
30% $30 copay
50% 50%
20% $40 copay
50% 50%
Hospital Precertification Required
Doctor Responsible
Associate Responsible**
Doctor Responsible
Associate Responsible**
Doctor Responsible
Associate Responsible**
Total OOPM (Medical & Prescription)
Individual Family
$6,750 $13,500
$13,500 $27,000
$6,750 $13,500
$13,500 $27,000
$6,750 $13,500
$13,500 $27,000
CVS / Caremark
Prescription Coverage
Retail
30-Day Supply
Once deductible is met, you pay
Generic
20%
Not Covered
$25 copay
Not Covered
$15 copay
Not Covered
Preferred Brand
20%
30% (Min:$40,Max:$500)
20% (Min:$30,Max:$500)
Non-Preferred
20%
30% (Min:$60,Max:$500)
20% (Min:$50,Max:$500)
Specialty
20%, to $500
30% (Max:$500)
20% (Max:$500)
Mail Order / Maintenance Choice 90-day Supply
Once deductible is met, you pay
Generic
20%
Not Covered
$45 copay
Not Covered
$25 copay
Not Covered
Preferred Brand
20%
30% (Min:$75,Max:$500)
20% (Min:$55,Max:$500)
Non-Preferred
20%
30% (Min:$115,Max:$500)
20% (Min:$95,Max:$500)
Specialty
20%, to $500
30% (Max:$500)
20% (Max:$500)
* May be subject to certain limitations, separate deductibles, copays, plan limits, or lifetime limits.
** $300 penalty applies for non-compliance.
*** One annual routine mammogram is covered in full at an in-network facility.
**** Benefits may be subject to separate deductibles, copay and limitations. Details about coverage of specific services can be
found in the summary plan description and plan documents.
RETURN TO INDEX
Applied Choices – 2019 11
