
Page 5 - NickCo Hospitality_2019 EE Benefits Guide_Mgmt_Working_11.27.pub
P. 5
BENEFITS
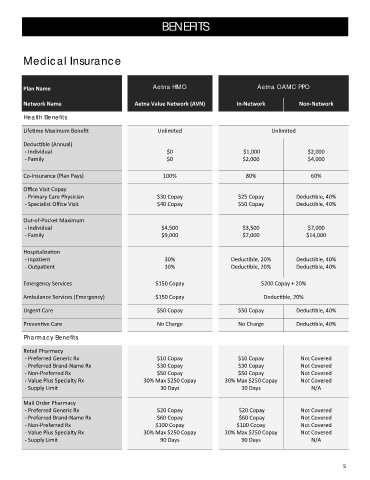
Medical Insurance
Plan Name Aetna HMO Aetna OAMC PPO
Network Name Aetna Value Network (AVN) In‐Network Non‐Network
Health Benefits
Life me Maximum Benefit Unlimited Unlimited
Deduc ble (Annual)
‐ Individual $0 $1,000 $2,000
‐ Family $0 $2,000 $4,000
Co‐Insurance (Plan Pays) 100% 80% 60%
Office Visit Copay
‐ Primary Care Physician $30 Copay $25 Copay Deduc ble, 40%
‐ Specialist Office Visit $40 Copay $50 Copay Deduc ble, 40%
Out‐of‐Pocket Maximum
‐ Individual $4,500 $3,500 $7,000
‐ Family $9,000 $7,000 $14,000
Hospitaliza on
‐ Inpa ent 30% Deduc ble, 20% Deduc ble, 40%
‐ Outpa ent 30% Deduc ble, 20% Deduc ble, 40%
Emergency Services $150 Copay $200 Copay + 20%
Ambulance Services (Emergency) $150 Copay Deduc ble, 20%
Urgent Care $50 Copay $50 Copay Deduc ble, 40%
Preven ve Care No Charge No Charge Deduc ble, 40%
Pharmacy Benefits
Retail Pharmacy
‐ Preferred Generic Rx $10 Copay $10 Copay Not Covered
‐ Preferred Brand‐Name Rx $30 Copay $30 Copay Not Covered
‐ Non‐Preferred Rx $50 Copay $50 Copay Not Covered
‐ Value Plus Specialty Rx 30% Max $250 Copay 30% Max $250 Copay Not Covered
‐ Supply Limit 30 Days 30 Days N/A
Mail Order Pharmacy
‐ Preferred Generic Rx $20 Copay $20 Copay Not Covered
‐ Preferred Brand‐Name Rx $60 Copay $60 Copay Not Covered
‐ Non‐Preferred Rx $100 Copay $100 Copay Not Covered
‐ Value Plus Specialty Rx 30% Max $250 Copay 30% Max $250 Copay Not Covered
‐ Supply Limit 90 Days 90 Days N/A
5