
Page 7 - JFSLA - Benefits Guide 2018-2019 - FINAL
P. 7
Benefits
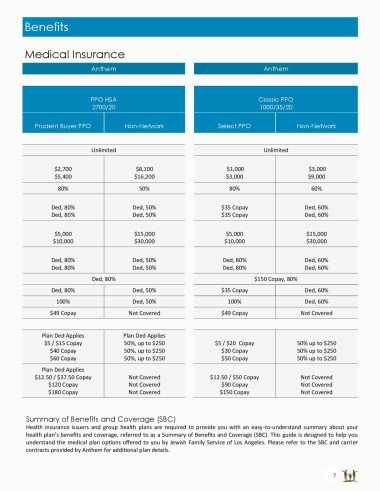
Medical Insurance
Anthem Anthem
PPO HSA Classic PPO
2700/20 1000/35/20
Prudent Buyer PPO Non-Network Select PPO Non-Network
Unlimited Unlimited
$2,700 $8,100 $1,000 $3,000
$5,400 $16,200 $3,000 $9,000
80% 50% 80% 60%
Ded, 80% Ded, 50% $35 Copay Ded, 60%
Ded, 80% Ded, 50% $35 Copay Ded, 60%
$5,000 $15,000 $5,000 $15,000
$10,000 $30,000 $10,000 $30,000
Ded, 80% Ded, 50% Ded, 80% Ded, 60%
Ded, 80% Ded, 50% Ded, 80% Ded, 60%
Ded, 80% $150 Copay, 80%
Ded, 80% Ded, 50% $35 Copay Ded, 60%
100% Ded, 50% 100% Ded, 60%
$49 Copay Not Covered $49 Copay Not Covered
Plan Ded Applies Plan Ded Applies
$5 / $15 Copay 50%, up to $250 $5 / $20 Copay 50% up to $250
$40 Copay 50%, up to $250 $30 Copay 50% up to $250
$60 Copay 50%, up to $250 $50 Copay 50% up to $250
Plan Ded Applies
$12.50 / $37.50 Copay Not Covered $12.50 / $50 Copay Not Covered
$120 Copay Not Covered $90 Copay Not Covered
$180 Copay Not Covered $150 Copay Not Covered
Summary of Benefits and Coverage (SBC)
Health insurance issuers and group health plans are required to provide you with an easy-to-understand summary about your
health plan’s benefits and coverage, referred to as a Summary of Benefits and Coverage (SBC). This guide is designed to help you
understand the medical plan options offered to you by Jewish Family Service of Los Angeles. Please refer to the SBC and carrier
contracts provided by Anthem for additional plan details.
7