
Page 4 - Dynacraft Benefit Summary 2020_Executives
P. 4
Benefits
Medical Insurance
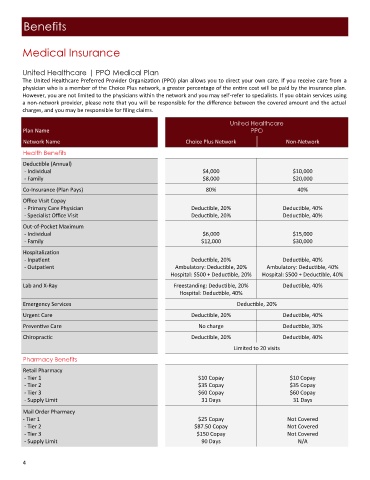
United Healthcare | PPO Medical Plan
The United Healthcare Preferred Provider Organization (PPO) plan allows you to direct your own care. If you receive care from a
physician who is a member of the Choice Plus network, a greater percentage of the entire cost will be paid by the insurance plan.
However, you are not limited to the physicians within the network and you may self-refer to specialists. If you obtain services using
a non‐network provider, please note that you will be responsible for the difference between the covered amount and the actual
charges, and you may be responsible for filing claims.
United Healthcare
Plan Name PPO
Network Name Choice Plus Network Non-Network
Health Benefits
Deductible (Annual)
- Individual $4,000 $10,000
- Family $8,000 $20,000
Co-Insurance (Plan Pays) 80% 40%
Office Visit Copay
- Primary Care Physician Deductible, 20% Deductible, 40%
- Specialist Office Visit Deductible, 20% Deductible, 40%
Out-of-Pocket Maximum
- Individual $6,000 $15,000
- Family $12,000 $30,000
Hospitalization
- Inpatient Deductible, 20% Deductible, 40%
- Outpatient Ambulatory: Deductible, 20% Ambulatory: Deductible, 40%
Hospital: $500 + Deductible, 20% Hospital: $500 + Deductible, 40%
Lab and X-Ray Freestanding: Deductible, 20% Deductible, 40%
Hospital: Deductible, 40%
Emergency Services Deductible, 20%
Urgent Care Deductible, 20% Deductible, 40%
Preventive Care No charge Deductible, 30%
Chiropractic Deductible, 20% Deductible, 40%
Limited to 20 visits
Pharmacy Benefits
Retail Pharmacy
- Tier 1 $10 Copay $10 Copay
- Tier 2 $35 Copay $35 Copay
- Tier 3 $60 Copay $60 Copay
- Supply Limit 31 Days 31 Days
Mail Order Pharmacy
- Tier 1 $25 Copay Not Covered
- Tier 2 $87.50 Copay Not Covered
- Tier 3 $150 Copay Not Covered
- Supply Limit 90 Days N/A
4