
Page 20 - FSSI EE Guide 07-20 - CA
P. 20
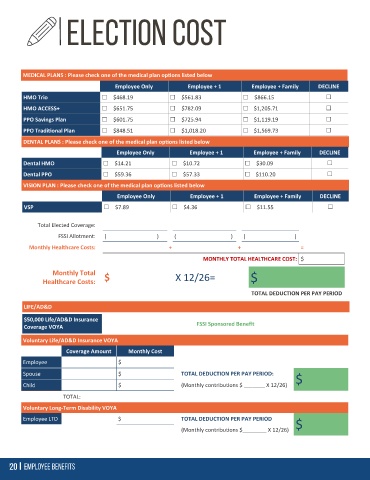
MEDICAL PLANS : Please check one of the medical plan options listed below
Employee Only Employee + 1 Employee + Family DECLINE
HMO Trio $468.19 $561.83 $866.15
HMO ACCESS+ $651.75 $782.09 $1,205.71
PPO Savings Plan $601.75 $725.94 $1,119.19
PPO Traditional Plan $848.51 $1,018.20 $1,569.73
DENTAL PLANS : Please check one of the medical plan options listed below
Employee Only Employee + 1 Employee + Family DECLINE
Dental HMO $14.21 $10.72 $30.09
Dental PPO $59.36 $57.33 $110.20
VISION PLAN : Please check one of the medical plan options listed below
Employee Only Employee + 1 Employee + Family DECLINE
VSP $7.89 $4.36 $11.55
Total Elected Coverage:
FSSI Allotment: ( ) ( ) ( )
Monthly Healthcare Costs: + + =
MONTHLY TOTAL HEALTHCARE COST: $
Monthly Total
Healthcare Costs: $ X 12/26= $
TOTAL DEDUCTION PER PAY PERIOD
LIFE/AD&D
$50,000 Life/AD&D Insurance
Coverage VOYA FSSI Sponsored Benefit
Voluntary Life/AD&D Insurance VOYA
Coverage Amount Monthly Cost
Employee $
Spouse $ TOTAL DEDUCTION PER PAY PERIOD:
$
Child $ (Monthly contributions $ _______ X 12/26)
TOTAL:
Voluntary Long-Term Disability VOYA
Employee LTD $ TOTAL DEDUCTION PER PAY PERIOD
$
(Monthly contributions $________ X 12/26)