
Page 8 - FSSI EE Guide 07-20 - CA
P. 8
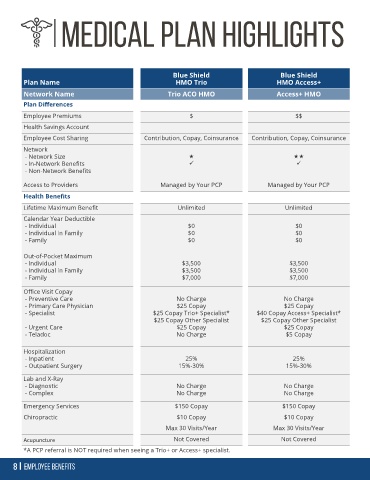
Blue Shield Blue Shield
Plan Name HMO Trio HMO Access+
Network Name Trio ACO HMO Access+ HMO
Plan Differences
Employee Premiums $ $$
Health Savings Account
Employee Cost Sharing Contribution, Copay, Coinsurance Contribution, Copay, Coinsurance
Network
- Network Size
- In-Network Benefits ✓ ✓
- Non-Network Benefits
Access to Providers Managed by Your PCP Managed by Your PCP
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Calendar Year Deductible
- Individual $0 $0
- Individual in Family $0 $0
- Family $0 $0
Out-of-Pocket Maximum
- Individual $3,500 $3,500
- Individual in Family $3,500 $3,500
- Family $7,000 $7,000
Office Visit Copay
- Preventive Care No Charge No Charge
- Primary Care Physician $25 Copay $25 Copay
- Specialist $25 Copay Trio+ Specialist* $40 Copay Access+ Specialist*
$25 Copay Other Specialist $25 Copay Other Specialist
- Urgent Care $25 Copay $25 Copay
- Teladoc No Charge $5 Copay
Hospitalization
- Inpatient 25% 25%
- Outpatient Surgery 15%-30% 15%-30%
Lab and X-Ray
- Diagnostic No Charge No Charge
- Complex No Charge No Charge
Emergency Services $150 Copay $150 Copay
Chiropractic $10 Copay $10 Copay
Max 30 Visits/Year Max 30 Visits/Year
Acupuncture Not Covered Not Covered
*A PCP referral is NOT required when seeing a Trio+ or Access+ specialist.