
Page 7 - Confie Benefits Guide
P. 7
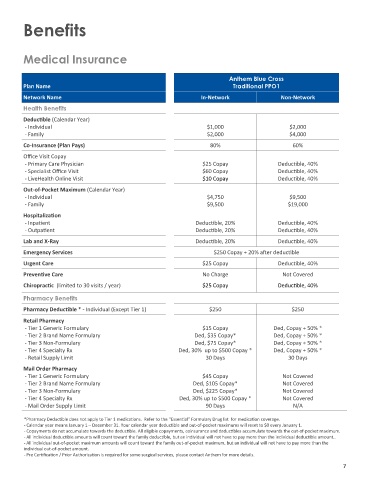
Benefits
Medical Insurance
Anthem Blue Cross
Plan Name Traditional PPO1
Network Name In-Network Non-Network
Health Benefits
Deductible (Calendar Year)
- Individual $1,000 $2,000
- Family $2,000 $4,000
Co-Insurance (Plan Pays) 80% 60%
Office Visit Copay
- Primary Care Physician $25 Copay Deductible, 40%
- Specialist Office Visit $60 Copay Deductible, 40%
- LiveHealth Online Visit $10 Copay Deductible, 40%
Out-of-Pocket Maximum (Calendar Year)
- Individual $4,750 $9,500
- Family $9,500 $19,000
Hospitalization
- Inpatient Deductible, 20% Deductible, 40%
- Outpatient Deductible, 20% Deductible, 40%
Lab and X-Ray Deductible, 20% Deductible, 40%
Emergency Services $250 Copay + 20% after deductible
Urgent Care $25 Copay Deductible, 40%
Preventive Care No Charge Not Covered
Chiropractic (limited to 30 visits / year) $25 Copay Deductible, 40%
Pharmacy Benefits
Pharmacy Deductible * - Individual (Except Tier 1) $250 $250
Retail Pharmacy
- Tier 1 Generic Formulary $15 Copay Ded, Copay + 50% *
- Tier 2 Brand Name Formulary Ded, $35 Copay* Ded, Copay + 50% *
- Tier 3 Non-Formulary Ded, $75 Copay* Ded, Copay + 50% *
- Tier 4 Specialty Rx Ded, 30% up to $500 Copay * Ded, Copay + 50% *
- Retail Supply Limit 30 Days 30 Days
Mail Order Pharmacy
- Tier 1 Generic Formulary $45 Copay Not Covered
- Tier 2 Brand Name Formulary Ded, $105 Copay* Not Covered
- Tier 3 Non-Formulary Ded, $225 Copay* Not Covered
- Tier 4 Specialty Rx Ded, 30% up to $500 Copay * Not Covered
- Mail Order Supply Limit 90 Days N/A
*Pharmacy Deductible does not apply to Tier 1 medications. Refer to the “Essential” Formulary Drug list for medication coverage.
- Calendar year means January 1 – December 31. Your calendar year deductible and out-of-pocket maximums will reset to $0 every January 1.
- Copayments do not accumulate towards the deductible. All eligible copayments, coinsurance and deductibles accumulate towards the out-of-pocket maximum.
- All individual deductible amounts will count toward the family deductible, but an individual will not have to pay more than the individual deductible amount..
- All individual out-of-pocket maximum amounts will count toward the family out-of-pocket maximum, but an individual will not have to pay more than the
individual out-of-pocket amount.
- Pre Certification / Prior Authorization is required for some surgical services, please contact Anthem for more details.
7