
Page 30 - New Hire Kit (Union)
P. 30
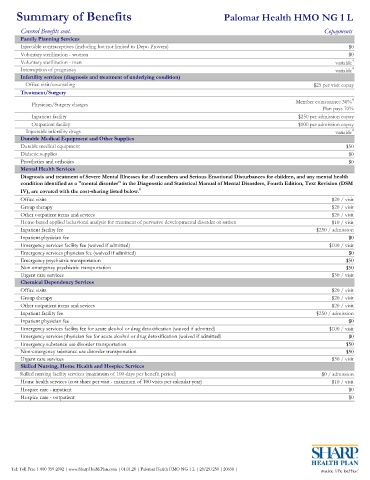
Summary of Benefits Palomar Health HMO NG 1 L
Covered Benefits cont. Copayments
Family Planning Services
Injectable contraceptives (including but not limited to Depo Provera) $0
Voluntary sterilization - women $0
Voluntary sterilization - men variable 4
Interruption of pregnancy variable 4
Infertility services (diagnosis and treatment of underlying condition)
Office visit/counseling $25 per visit copay
Treatment/Surgery
Physician/Surgery charges Member coinsurance 30% 4
Plan pays 70%
Inpatient facility $250 per admission copay
Outpatient facility $100 per admission copay
Injectable infertility drugs variable 4
Durable Medical Equipment and Other Supplies
Durable medical equipment $50
Diabetic supplies $0
Prosthetics and orthotics $0
Mental Health Services
Diagnosis and treatment of Severe Mental Illnesses for all members and Serious Emotional Disturbances for children, and any mental health
condition identified as a "mental disorder" in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM
IV), are covered with the cost-sharing listed below. 6
Office visits $20 / visit
Group therapy $20 / visit
Other outpatient items and sevices $20 / visit
Home-based applied behavioral analysis for treatment of pervasive developmental disorder or autism $10 / visit
Inpatient facility fee $250 / admission
Inpatient physician fee $0
Emergency services facility fee (waived if admitted) $100 / visit
Emergency services physician fee (waived if admitted) $0
Emergency psychiatric transportation $50
Non-emergency psychiatric transportation $50
Urgent care services $30 / visit
Chemical Dependency Services
Office visits $20 / visit
Group therapy $20 / visit
Other outpatient items and sevices $20 / visit
Inpatient facility fee $250 / admission
Inpatient physician fee $0
Emergency services facility fee for acute alcohol or drug detoxification (waived if admitted) $100 / visit
Emergency services physician fee for acute alcohol or drug detoxification (waived if admitted) $0
Emergency substance use disorder transportation $50
Non-emergency substance use disorder transportation $50
Urgent care services $30 / visit
Skilled Nursing, Home Health and Hospice Services
Skilled nursing facility services (maximum of 100 days per benefit period) $0 / admission
Home health services (cost share per visit - maximum of 100 visits per calendar year) $10 / visit
Hospice care - inpatient $0
Hospice care - outpatient $0
Tel: Toll-Free 1-800-359-2002 | www.SharpHealthPlan.com | 01.01.20 | Palomar Health HMO NG 1 L | 20/25/250 | 20638 |