
Page 44 - New Hire Kit (Union)
P. 44
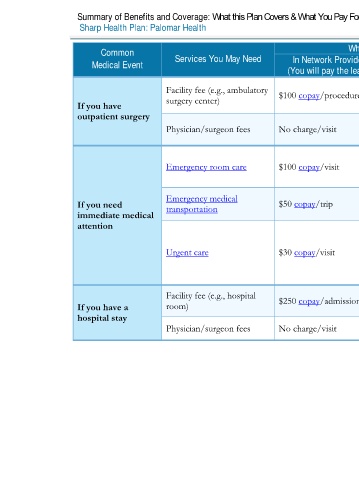
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2020 – 12/31/2020
Sharp Health Plan: Palomar Health Coverage for: Individual / Family | Plan Type: HMO
Common Services You May Need What You Will Pay Limitations, Exceptions, & Other
Medical Event In Network Provider Out-of-Network Provider Important Information
(You will pay the least) (You will pay the most)
Facility fee (e.g., ambulatory $100 copay/procedure Not covered
surgery center)
If you have
outpatient surgery Preauthorization is required.
Physician/surgeon fees No charge/visit Not covered
Cost sharing waived if admitted to the
Emergency room care $100 copay/visit $100 copay/visit
hospital.
Emergency medical
If you need transportation $50 copay/trip $50 copay/trip None
immediate medical
attention Services must be approved by your primary
care provider and received at urgent care
facilities affiliated with your Plan Medical
Urgent care $30 copay/visit $30 copay/visit
Group. Out-of-Network services are
covered only when you are outside of the
Service Area for your Plan Network.
Facility fee (e.g., hospital $250 copay/admission $250 copay/admission
If you have a room) Preauthorization is required for non-
emergency services. Out-of-network services
hospital stay are covered for emergency care only.
Physician/surgeon fees No charge/visit No charge/visit
3 of 11
Palomar Health HMO NG 1 L / ACCH15_40 / VSA8