
Page 2 - Cal Resite Care - 2020 Open Enrollment Action Guide
P. 2
MEDICAL BENEFITS
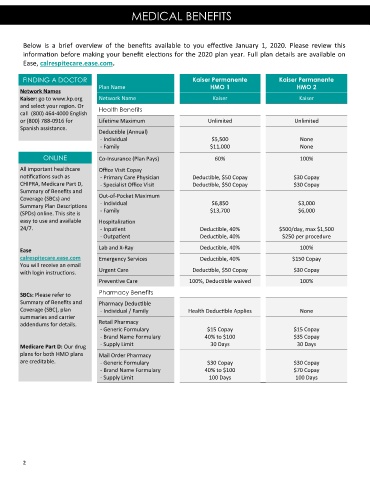
Below is a brief overview of the benefits available to you effective January 1, 2020. Please review this
information before making your benefit elections for the 2020 plan year. Full plan details are available on
Ease, calrespitecare.ease.com.
FINDING A DOCTOR Kaiser Permanente Kaiser Permanente
Plan Name HMO 1 HMO 2
Network Names
Kaiser: go to www.kp.org Network Name Kaiser Kaiser
and select your region. Or Health Benefits
call (800) 464-4000 English
or (800) 788-0916 for Lifetime Maximum Unlimited Unlimited
Spanish assistance. Deductible (Annual)
- Individual $5,500 None
- Family $11,000 None
ONLINE Co-Insurance (Plan Pays) 60% 100%
All important healthcare Office Visit Copay
notifications such as - Primary Care Physician Deductible, $50 Copay $30 Copay
CHIPRA, Medicare Part D, - Specialist Office Visit Deductible, $50 Copay $30 Copay
Summary of Benefits and
Coverage (SBCs) and Out-of-Pocket Maximum
- Individual $6,850 $3,000
Summary Plan Descriptions
(SPDs) online. This site is - Family $13,700 $6,000
easy to use and available Hospitalization
24/7. - Inpatient Deductible, 40% $500/day, max $1,500
- Outpatient Deductible, 40% $250 per procedure
Ease Lab and X-Ray Deductible, 40% 100%
calrespitecare.ease.com Emergency Services Deductible, 40% $150 Copay
You will receive an email
with login instructions. Urgent Care Deductible, $50 Copay $30 Copay
Preventive Care 100%, Deductible waived 100%
SBCs: Please refer to Pharmacy Benefits
Summary of Benefits and Pharmacy Deductible
Coverage (SBC), plan - Individual / Family Health Deductible Applies None
summaries and carrier
Retail Pharmacy
addendums for details.
- Generic Formulary $15 Copay $15 Copay
- Brand Name Formulary 40% to $100 $35 Copay
- Supply Limit 30 Days 30 Days
Medicare Part D: Our drug
plans for both HMO plans Mail Order Pharmacy
are creditable. - Generic Formulary $30 Copay $30 Copay
- Brand Name Formulary 40% to $100 $70 Copay
- Supply Limit 100 Days 100 Days
2