
Page 11 - Optima Tax EE Guide 01-20 CA
P. 11
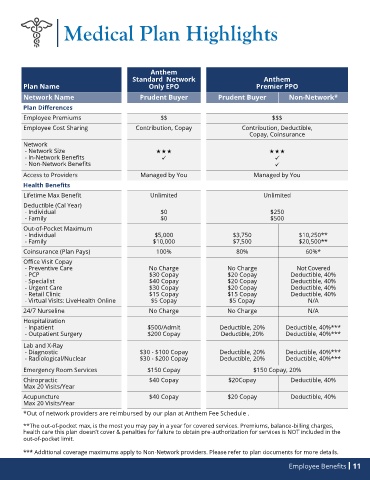
Medical Plan Highlights
Anthem
Standard Network Anthem
Plan Name Only EPO Premier PPO
Network Name Prudent Buyer Prudent Buyer Non-Network*
Plan Differences
Employee Premiums $$ $$$
Employee Cost Sharing Contribution, Copay Contribution, Deductible,
Copay, Coinsurance
Network
- Network Size
- In-Network Benefits ✓ ✓
- Non-Network Benefits ✓
Access to Providers Managed by You Managed by You
Health Benefits
Lifetime Max Benefit Unlimited Unlimited
Deductible (Cal Year)
- Individual $0 $250
- Family $0 $500
Out-of-Pocket Maximum
- Individual $5,000 $3,750 $10,250**
- Family $10,000 $7,500 $20,500**
Coinsurance (Plan Pays) 100% 80% 60%*
Office Visit Copay
- Preventive Care No Charge No Charge Not Covered
- PCP $30 Copay $20 Copay Deductible, 40%
- Specialist $40 Copay $20 Copay Deductible, 40%
- Urgent Care $30 Copay $20 Copay Deductible, 40%
- Retail Clinic $15 Copay $15 Copay Deductible, 40%
- Virtual Visits: LiveHealth Online $5 Copay $5 Copay N/A
24/7 Nurseline No Charge No Charge N/A
Hospitalization
- Inpatient $500/Admit Deductible, 20% Deductible, 40%***
- Outpatient Surgery $200 Copay Deductible, 20% Deductible, 40%***
Lab and X-Ray
- Diagnostic $30 - $100 Copay Deductible, 20% Deductible, 40%***
- Radiological/Nuclear $30 - $200 Copay Deductible, 20% Deductible, 40%***
Emergency Room Services $150 Copay $150 Copay, 20%
Chiropractic $40 Copay $20Copay Deductible, 40%
Max 20 Visits/Year
Acupuncture $40 Copay $20 Copay Deductible, 40%
Max 20 Visits/Year
*Out of network providers are reimbursed by our plan at Anthem Fee Schedule .
**The out-of-pocket max, is the most you may pay in a year for covered services. Premiums, balance-billing charges,
health care this plan doesn’t cover & penalties for failure to obtain pre-authorization for services is NOT included in the
out-of-pocket limit.
*** Additional coverage maximums apply to Non-Network providers. Please refer to plan documents for more details.
Employee Benefits 11