
Page 13 - Work Life and Benefits Booklet 2018 - SDC.END.pub
P. 13
13
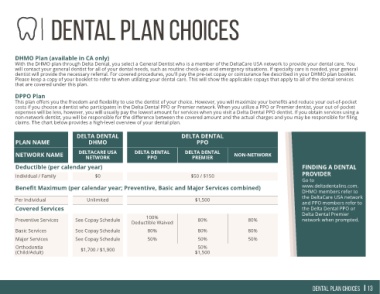
expenses will be less, however, you will usually pay the lowest amount for services when you visit a Delta Dental PPO dentist. If you obtain services using a
will contact your general dentist for all of your dental needs, such as routine check-ups and emergency situations. If specialty care is needed, your general
This plan offers you the freedom and flexibility to use the dentist of your choice. However, you will maximize your benefits and reduce your out-of-pocket
non-network dentist, you will be responsible for the difference between the covered amount and the actual charges and you may be responsible for filing
FINDING A DENTAL PROVIDER Go to www.deltadentalins.com. DHMO members refer to the DeltaCare USA network and PPO members refer to the Delta Dental PPO or Delta Dental Premier network when prompted. Dental Plan choices
dentist will provide the necessary referral. For covered procedures, you'll pay the pre-set copay or coinsurance fee described in your DHMO plan booklet.
With the DHMO plan through Delta Dental, you select a General Dentist who is a member of the DeltaCare USA network to provide your dental care. You
costs if you choose a dentist who participates in the Delta Dental PPO or Premier network. When you utilize a PPO or Premier dentist, your out-of-pocket
Please keep a copy of your booklet to refer to when utilizing your dental care. This will show the applicable copays that apply to all of the dental services
NON-NETWORK 80% 80% 50%
Dental Plan Choices
DELTA DENTAL PPO DELTA DENTAL PREMIER $50 / $150 $1,500 80% 80% 50% 50% $1,500
claims. The chart below provides a high-level overview of your dental plan.
DELTA DENTAL PPO 100% Deductible Waived 80% 50%
Benefit Maximum (per calendar year; Preventive, Basic and Major Services combined)
DELTA DENTAL DHMO DELTACARE USA NETWORK $0 Unlimited See Copay Schedule See Copay Schedule See Copay Schedule $1,700 / $1,900
DHMO Plan (available in CA only)
that are covered under this plan. DPPO Plan PLAN NAME NETWORK NAME Deductible (per calendar year) Individual / Family Per Individual Covered Services Preventive Services Basic Services Major Services Orthodontia (Child/Adult)