
Page 6 - KNCH Benefits Guide 2019 v3
P. 6
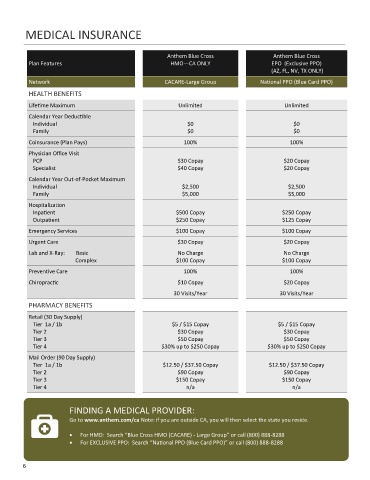
MEDICAL INSURANCE
Anthem Blue Cross Anthem Blue Cross
Plan Features HMO—CA ONLY EPO (Exclusive PPO)
(AZ, FL, NV, TX ONLY)
Network CACARE-Large Group National PPO (Blue Card PPO)
HEALTH BENEFITS
Lifetime Maximum Unlimited Unlimited
Calendar Year Deductible
Individual $0 $0
Family $0 $0
Coinsurance (Plan Pays) 100% 100%
Physician Office Visit
PCP $30 Copay $20 Copay
Specialist $40 Copay $20 Copay
Calendar Year Out-of-Pocket Maximum
Individual $2,500 $2,500
Family $5,000 $5,000
Hospitalization
Inpatient $500 Copay $250 Copay
Outpatient $250 Copay $125 Copay
Emergency Services $100 Copay $100 Copay
Urgent Care $30 Copay $20 Copay
Lab and X-Ray: Basic No Charge No Charge
Complex $100 Copay $100 Copay
Preventive Care 100% 100%
Chiropractic $10 Copay $20 Copay
30 Visits/Year 30 Visits/Year
PHARMACY BENEFITS
Retail (30 Day Supply)
Tier 1a / 1b $5 / $15 Copay $5 / $15 Copay
Tier 2 $30 Copay $30 Copay
Tier 3 $50 Copay $50 Copay
Tier 4 $30% up to $250 Copay $30% up to $250 Copay
Mail Order (90 Day Supply)
Tier 1a / 1b $12.50 / $37.50 Copay $12.50 / $37.50 Copay
Tier 2 $90 Copay $90 Copay
Tier 3 $150 Copay $150 Copay
Tier 4 n/a n/a
FINDING A MEDICAL PROVIDER:
Go to www.anthem.com/ca Note: if you are outside CA, you will then select the state you reside.
• For HMO: Search “Blue Cross HMO (CACARE) - Large Group” or call (800) 888-8288
• For EXCLUSIVE PPO: Search “National PPO (Blue Card PPO)” or call (800) 888-8288
6